Molecular feature-based classification of retroperitoneal liposarcoma: a prospective cohort study
- Department of Retroperitoneal Tumor Surgery, Peking University People’s Hospital, China
- Department of Retroperitoneal Tumor Surgery, Peking University International Hospital, China
- Department of Gastroenterology, Beijing Friendship Hospital, Capital Medical University, State Key Laboratory for Digestive Health, National Clinical Research Center for Digestive Disease, Beijing Digestive Disease Center, Beijing Key Laboratory for Precancerous Lesion of Digestive Disease, China
- Department of Biomedical Sciences, Humanitas University, Italy
eLife Assessment
This study presents a valuable and simplified classification system for predicting clinical outcomes of RPLS patients. The data were collected and analyzed using solid and validated methodology and can be used as a starting point for personalized treatment of RPLS. The work will be of interest to scientists working in the field of RPLS.
https://doi.org/10.7554/eLife.100887.3.sa0Significance of the findings:
Valuable: Findings that have theoretical or practical implications for a subfield
- Landmark
- Fundamental
- Important
- Valuable
- Useful
Strength of evidence:
Solid: Methods, data and analyses broadly support the claims with only minor weaknesses
- Exceptional
- Compelling
- Convincing
- Solid
- Incomplete
- Inadequate
During the peer-review process the editor and reviewers write an eLife Assessment that summarises the significance of the findings reported in the article (on a scale ranging from landmark to useful) and the strength of the evidence (on a scale ranging from exceptional to inadequate). Learn more about eLife Assessments
Abstract
Background:
Retroperitoneal liposarcoma (RPLS) is a critical malignant disease with various clinical outcomes. However, the molecular heterogeneity of RPLS was poorly elucidated, and few biomarkers were proposed to monitor its progression.
Methods:
RNA sequencing was performed on a training cohort of 88 RPLS patients to identify dysregulated genes and pathways using clusterProfiler. The GSVA algorithm was utilized to assess signaling pathway levels in each sample, and unsupervised clustering was employed to distinguish RPLS subtypes. Differentially expressed genes (DEGs) between RPLS subtypes were identified to construct a simplified dichotomous clustering via nonnegative matrix factorization. The feasibility of this classification was validated in a separate validation cohort (n=241) using immunohistochemistry (IHC) from the REtroperitoneal SArcoma Registry (RESAR). The study is registered with https://clinicaltrials.gov/ under number NCT03838718.
Results:
Cell cycle, DNA damage and repair, and metabolism were identified as the most aberrant biological processes in RPLS, enabling the division of RPLS patients into two distinct subtypes with unique molecular signatures, tumor microenvironment, clinical features, and outcomes (overall survival [OS] and disease-free survival [DFS]). A simplified RPLS classification based on representative biomarkers (LEP and PTTG1) demonstrated high accuracy (area under the curve [AUC]>0.99), with patients classified as LEP+ and PTTG1-, showing lower aggressive pathological composition ratio and fewer surgery times, along with better OS (HR = 0.41, p<0.001) and DFS (HR = 0.60, p=0.005).
Conclusions:
Our study provided an ever-largest gene expression landscape of RPLS and established an IHC-based molecular classification that was clinically relevant and cost-effective for guiding treatment decisions.
Funding:
This work was supported by grants from the Beijing Municipal Science and Technology Project (Z191100006619081), National Natural Science Foundation of China (82073390), and Young Elite Scientists Sponsorship Program (2023QNRC001). The study sponsors had no role in the design and preparation of this manuscript.
Clinical trial number:
eLife digest
Retroperitoneal liposarcoma (or RPLS for short) is a rare type of cancer that forms a tumor deep in the abdomen. Although it can be treated through surgery, results vary widely, and the cancer often returns. Determining which RPLS tumours are likely to respond well to treatment, and which are more aggressive, can be challenging. This is partly because many of the tumors appear similar under a microscope, making it difficult to identify those that might require more intense treatment.
For some types of cancer, researchers have started to overcome this problem by identifying molecular markers – specific genes, proteins and other molecules – that are unique to tumor cells. This allows for a better understanding of tumor behavior and helps pinpoint which treatments are most likely to be successful. However, the relevant molecular markers for RPLS remain unknown, preventing this precision medicine approach from being applied to this type of cancer.
To help close this gap, Xiao et al. studied the genetic activity of tumors from 88 RPLS patients to look for activity associated with more aggressive tumors. Analysis revealed two distinct groups of tumors. One group showed high activity of a gene known as LEP, which is involved in metabolism. Tumors with high LEP activity were less aggressive, with patients surviving longer and requiring fewer surgeries. The other tumor group showed high activity of a gene known as PTTG1, which plays a role in cell division and DNA repair. When overactive, these processes can make tumors grow and spread more quickly. In this group, tumors were more likely to return after surgery. Based on these findings, Xiao et al. developed a simple test using the two genes to classify tumors. When tested in a larger group of 241 patients, this method successfully sorted tumors into the two groups with more than 99% accuracy.
The findings of Xiao et al. suggest that the activity of LEP and PTTG1 could potentially be used as a molecular marker for identifying RPLS patients that might benefit from more intensive treatments. However, further research is required to confirm how reliable these markers are before they can be used to diagnose patients in the clinic.
Introduction
Retroperitoneal liposarcoma (RPLS) is a soft tissue sarcoma originating in the retroperitoneum with an insidious onset. Traditional surgical resection has been regarded as a primary and curable treatment strategy of RPLS for the past 50 years (Ecker et al., 2016). However, the anatomical complexity and biological properties of sarcoma brought great difficulty in achieving microscopically margin-negative resection, leading to a high postoperative recurrence rate in RPLS patients. During the past decade, scientists tried to improve the postoperative survival of RPLS patients by personalized surgical resection and neoadjuvant/adjuvant therapies, but the effect was not satisfactory (Littau et al., 2021; Gronchi et al., 2015; Gronchi et al., 2009; Gronchi and Pollock, 2013; Pisters, 2009).
Recently, precision medicine greatly enriched the therapeutic approaches and reformed the clinical decision-making chain of tumor diagnosis and treatment, prolonging the median survival of main tumor types 2–10 times (Kam et al., 2021; Zeng and Jin, 2022; Alifrangis et al., 2019; Frese et al., 2021). Biomarker-based patient stratification and targeted therapy together make up the kernel of precision medicine, which is intrinsically based on the molecular profiling of cancers. However, our knowledge of the molecular features of RPLS is limited, and few clinically applicable molecular biomarkers and targeted drugs are available for RPLS treatment. Only sporadic molecules such as CDK4 (Pilotti et al., 2000), MDM2 (Binh et al., 2005), AURK4 (Yen et al., 2019), and CCNDBP1 (Yang et al., 2021) have been reported as prognostic and diagnostic biomarkers, but these biomarkers were poorly represented and verified. Therefore, it is crucial to reveal the molecular landscape of RPLS and explore a feasible classification for its diagnosis and treatment.
Here, we conducted a comprehensive investigation into the molecular characteristics of RPLS through the delineation of the largest gene expression landscape ever assembled for this rare disease entity. By identifying both RPLS-specific genes and prognostic biomarkers, we unveiled their intricate relationships with clinical parameters. Our findings revealed the existence of two distinct molecular subtypes within all RPLS patients, characterized by diverse pathological compositions, enriched signaling pathways, and varying clinical outcomes. This highlights the limitations of relying solely on traditional pathological classification for surgical decision-making in certain cases where patients exhibit favorable histological features but poor prognoses, emphasizing the pivotal role of molecular subtyping in guiding individualized treatment strategies and enhancing patient management. To facilitate practical application in clinical settings, we developed a simplified RPLS classification system based on key biomarkers (LEP and PTTG1) representative of each subtype. Notably, this classification scheme was validated in a larger cohort of RPLS patients through immunohistochemistry (IHC) assays (Figure 1), laying the groundwork for precise surgical interventions guided by molecular insights in the realm of RPLS treatment.
Figure 1
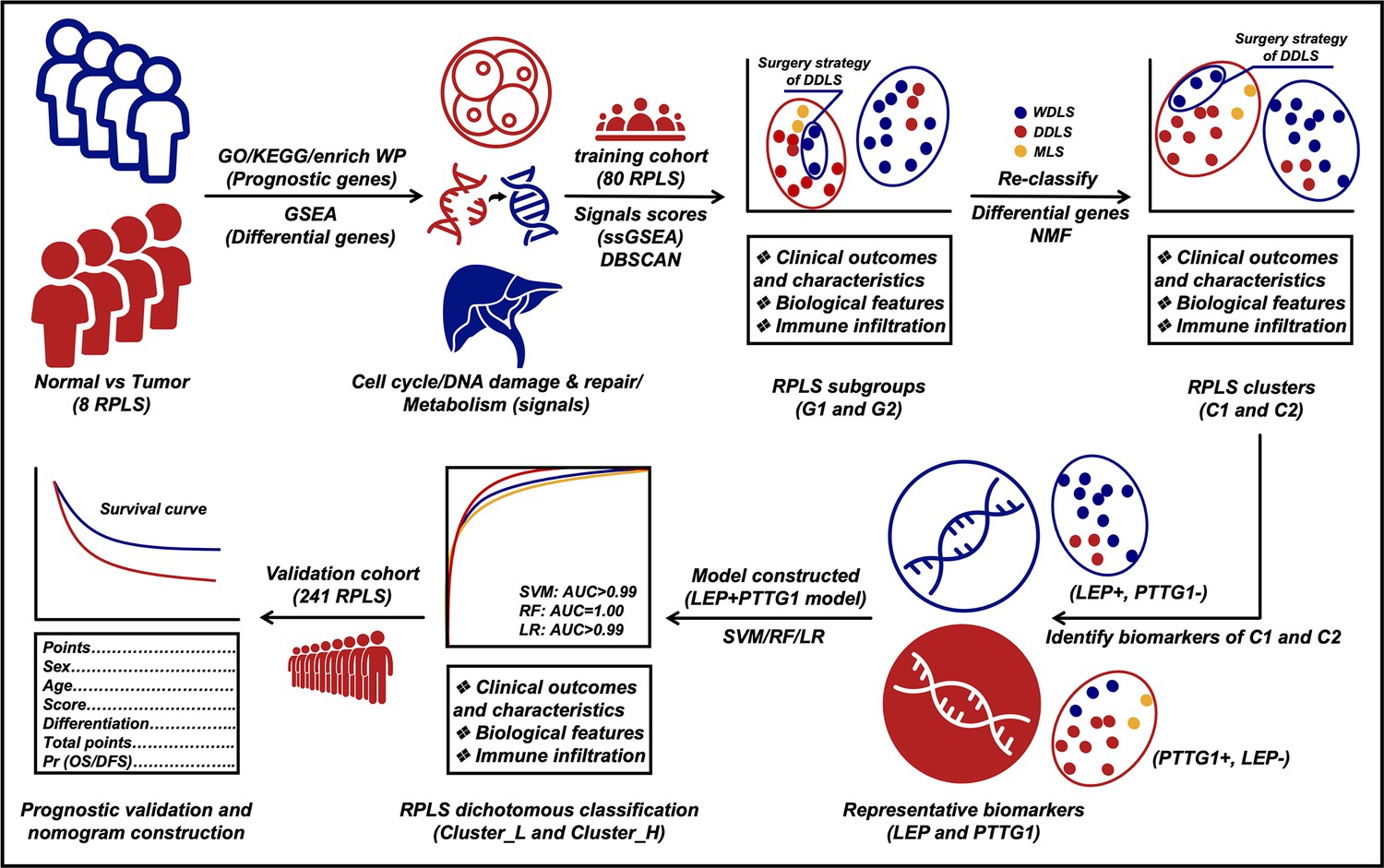
Flow diagram of exploring retroperitoneal liposarcoma (RPLS) dichotomous classification.
Materials and methods
Patients and tissue specimens
Request a detailed protocolPatients who were diagnosed with RPLS amenable to surgical resection were eligible for the study. The RPLS histology was confirmed according to the WHO criteria done on biopsy or surgical specimen by a dedicated sarcoma pathologist. Exclusion criteria comprised age <18 years, severe psychiatric disorders impairing informed consent or study compliance, and inability to ensure adequate follow-up. Tumor specimens from 88 RPLS patients (training cohort 1, Supplementary file 1; training cohort 2, Supplementary file 2) and another cohort of 241 RPLS patients (validation cohort, Supplementary file 3) were obtained from our local hospital. These cohorts are sourced from REtroperitoneal SArcoma Registry (RESAR, NCT03838718). All the patients underwent curative resection from January 2015 to May 2019. RPLS tissue specimens were snap-frozen in liquid nitrogen within 1 hr and then stored in a –80°C refrigerator before use. Clinical information was collected from the medical records, and no patient had undergone previous chemotherapy or radiotherapy. Overall survival (OS) was defined as the interval between the latest surgery and death from tumors or between the latest surgery and the last observation taken for surviving patients. Disease-free survival (DFS) was defined as the interval between the latest surgery and diagnosis of relapse or death. Informed consent for surgical procedures and specimen collection was obtained from each patient. This study has been reported in line with the REMARK criteria (McShane et al., 2005). The data of the external validation cohort (GSE30929) was downloaded from GEO (https://www.ncbi.nlm.nih.gov/geo/).
RNA sequencing, primary data processing, and analysis
Request a detailed protocolTotal RNA was extracted from training cohort 1 (Supplementary file 4) and training cohort 2 (Supplementary file 2) using TRIzol Reagent (Invitrogen). RNA degradation and contamination were monitored with 1% agarose gel. RNA purity was checked by the NanoPhotometer spectrophotometer (IMPLEN, Los Angeles, CA, USA). RNA concentration was measured using the Qubit RNA Assay Kit with the Qubit 2.0 Fluorometer (Life Technologies, CA, USA). RNA integrity was assessed using the RNA Nano 6000 Assay Kit of the Agilent Bioanalyzer 2100 System (Agilent Technologies, CA, USA).
A total amount of 3–5 µg RNA per sample was used as input material for the RNA library. Sequencing libraries were generated using NEBNext Multiplex Small RNA Library Prep Set for Illumina (NEB, USA) following the manufacturer’s recommendations, and index codes were added to attribute sequences to each sample. The clustering of the index-coded samples was performed on a cBot Cluster Generation System using TruSeq SR Cluster Kit v3-cBot-HS (Illumina). After cluster generation, the strand-specific cDNA was sequenced on an Illumina NovaSeq 6000 platform, and single-end reads were generated (Novogene Bioinformatic Technology, Beijing, China).
FPKMs of mRNAs and noncoding RNAs in each sample were calculated by Cuffdiff (v2.1.1). FPKMs were calculated based on the length of the fragments and read counts mapped to this fragment. These sequencing data have been deposited at the Open Archive for Miscellaneous Data (OMIX) database of China National Center for Bioinformation (CNCB) under the accession number OMIX002786.
Identification of differential genes
Request a detailed protocolGene difference analysis was performed to determine the differential genes (differentially expressed genes [DEGs]). An adjusted false discovery rate (FDR)<0.05 and |log2FC|>0.585 were considered significant. This process was conducted with the R package ‘limma’.
Identification of prognostic genes
Request a detailed protocolCox univariate regression analysis was used to screen the prognostic genes of RPLS. Results of p<0.05 were considered significant. This process was conducted with the R package ‘survival’.
GSEA and immune infiltrate analysis
Request a detailed protocolGene set enrichment analysis (GSEA) was performed in the tumor and normal groups to explore the biological signaling pathways. Pathway annotation files were downloaded from the MSigDB (https://www.gsea-msigdb.org/gsea/index.jsp) platform. This process was conducted by the GSEA R package to elucidate the representative HALLMARK and REACTOME pathways enriched in RPLS patients. Immunocyte infiltration (immune score and stromal score) was measured by the Estimation of STromal and Immune cells in Malignant Tumor tissues using Expression data (ESTIMATE) algorithm. This process was completed via the ‘estimate’ R package.
Functional annotation
Request a detailed protocolFunctional enrichment analyses were performed to elucidate the possible biological processes and signaling pathways of the prognostic genes. Gene Ontology (GO) and Kyoto Encyclopedia of Gene and Genomes (KEGG) analyses were conducted by the R package ‘clusterProfiler’, and the FDR<0.05 was considered significantly enriched.
Consensus clustering with t-SNE
Request a detailed protocolAfter evaluating the relative abundance level of related pathways, the Euclidean distance was calculated between any two samples and condensed into two-dimensional points using t-distributed stochastic neighbor embedding (t-SNE) (Guo et al., 2019a) and subsequently visualized automatically with the density-based spatial clustering of applications with noise (DBSCAN) algorithm. This consensus clustering was conducted with the R packages ‘Rtsne’ and ‘dbscan’.
Consensus clustering with NMF
Request a detailed protocolNonnegative matrix factorization (NMF) was used to perform RPLS subtyping. Specifically, NMF was applied to gene expression matrix A which contained gene sets of major signaling pathways and prognostic genes. Matrix A was factorized into two nonnegative matrices W and H. Repeated factorization of matrix A was performed, and its outputs were aggregated to obtain consensus clustering of RPLS samples. The optimal number of subtypes was selected according to cophenetic, dispersion, and silhouette coefficients. This consensus clustering was conducted with the R package ‘NMF’.
Construction of machine learning models
Request a detailed protocolMachine learning models based on biomarkers were constructed by logistic regression (LR), support vector machine (SVM), and random forest (RF). These models were specifically tailored to analyze biomarker data in order to predict clinical outcomes in surgical patients.
LR is a statistical method that establishes a relationship between a set of independent variables and a binary outcome. It calculates the probability of an event occurring based on the six to seven input features derived from biomarkers relevant to the surgical patient. SVM is a supervised learning algorithm that categorizes data points by identifying the optimal hyperplane that separates distinct classes within a high-dimensional space. This approach effectively maps biomarker data into a multidimensional space to facilitate accurate classification of patient outcomes. RF is an ensemble learning technique that generates multiple decision trees during training and aggregates the results to make predictions. By leveraging this method, we can enhance predictive accuracy by mitigating overfitting and increasing model robustness when analyzing biomarker-driven patient data.
The performance of these machine learning models was assessed using the area under the curve (AUC) metric. A higher AUC value indicates superior discriminatory power of the model in distinguishing different clinical outcomes. An AUC value closer to 1.0 signifies strong predictive capability, while 0.5 indicates no discriminatory ability at all. By evaluating the AUC values generated by LR, SVM, and RF models, clinicians can identify which algorithm yields the most reliable predictions based on biomarker profiles for surgical patients.
Immunohistochemistry
Request a detailed protocolThe protocol was performed as previously described (Li et al., 2022). In brief, the LEP and PTTG1 antibodies for IHC were purchased from Proteintech (Cat No: bs-0409R and bs-1881R). With deparaffinization for 15 min×3 in dimethylbenzene and routine hydration, the tissues were soaked in phosphate-buffered saline for 10 min and then performed high-pressure antigen retrieval (Tris-EDTA, pH = 9.0) for 2.5 min. After being treated with a 3% endogenous catalase blocker (ZSBIO, PV-6000) for 10 min, the tissues were incubated in goat serum (ZSBIO, ZLI-9022) for the blocking of nonspecific reaction and then incubated with primary antibody (LEP = 1:300 and PTTG1=1:300) at 4°C overnight. The next day, tissues were washed and incubated with goat anti-rabbit secondary antibody (ZSBIO, PV-9000) for 1 hr at room temperature, then washed and stained with DAB reagents (ZSBIO, ZLI-9018). Then, hematoxylin staining, 1% hydrochloric acid alcohol differentiation, ammonia water anti-blue, and neutral gum sealing.
The IHC results were evaluated by pathologists, and the staining extent was scored as 0–100%. The intensity score was defined as negative, low-expression, medium-expression, and high-expression, which were documented as 0, 1, 2, and 3, respectively. The final scores were calculated by the formula: IHC score = Staining extent score × Staining intensity score.
Statistical methods
Request a detailed protocolR software (v4.1.3) was used in this study. For quantitative variables, differences between the two groups and among multiple groups were analyzed by Wilcoxon’s test and one-way analysis of variance (ANOVA), respectively. For categorical variables, groups were compared by the use of a chi-square test. Survival curves were determined by the log-rank test. The clinicopathological features and levels of immune infiltration were conducted by Wilcoxon’s test. A difference of p<0.05 indicated statistical significance unless specified otherwise.
Results
Baseline characteristics were shown in Table 1. Of 329 RPLS patients, 88 in training cohort and 241 in validation cohort. No statistically significant differences were found in the age, sex, pathology, surgery times, tumor size, and multilocation between the two cohorts (p>0.05). In validation cohort, the IHC scores of LEP and PTTG1 were 1.62 (0.820) and 0.830 (0.75), respectively.
Table 1
Baseline characteristics of training cohort and validation cohort.
| Training cohort (N=80)* | Validation cohort (N=241) | p-Value | |
|---|---|---|---|
| Age (years) | 56.34 (11.14)† | 55.11 (10.80) † | 0.384 |
| Sex | |||
| Male | 37 (46.25) | 118 (48.96) | 0.674 |
| Female | 43 (53.75) | 123 (51.04) | |
| Pathology | |||
| WDLS | 29 (36.25) | 75 (31.12) | 0.078 |
| DDLS | 48 (60.00) | 144 (59.75) | |
| MLS and PLS | 3 (3.75) | 5 (2.07) | |
| NR | 0 (0) | 17 (7.06) | |
| Surgery times ‡ | |||
| 0–1 | 50 (62.50) | 143 (59.34) | 0.834 |
| 2–3 | 21 (26.25) | 73 (30.29) | |
| 4–7 | 9 (11.25) | 24 (9.96) | |
| NR | 0 (0) | 1 (0.41) | |
| Tumor size | |||
| All | 18.65 (8.70)† | 16.90 (7.94)† | 0.101 |
| <18 cm | 40 (50.00) | 135 (56.02) | 0.095 |
| >18 cm | 39 (48.75) | 92 (38.17) | |
| NR | 1 (1.25) | 14 (5.81) | |
| Multilocation | |||
| Yes | 52 (65.00) | 153 (63.49) | 0.081 |
| No | 28 (35.00) | 74 (30.71) | |
| NR | 0 (0) | 14 (5.80) | |
| MDM2 score | |||
| 0 | 11 (13.75) | NA | NA |
| 1 | 12 (15.00) | NA | |
| 2 | 39 (48.75) | NA | |
| 3 | 5 (6.25) | NA | |
| 4 | 9 (11.25) | NA | |
| NR | 4 (5.00) | NA | |
| LEP score | NA | 1.62 (0.82)† | NA |
| LEP strength | |||
| 0 | NA | 10 (4.15) | NA |
| 1 | NA | 39 (16.18) | |
| 2 | NA | 74 (30.71) | |
| 3 | NA | 115 (47.72) | |
| NR | NA | 3 (1.24) | |
| PTTG1 score | NA | 0.83 (0.75)† | NA |
| PTTG1 strength | |||
| 0 | NA | 38 (15.77) | NA |
| 1 | NA | 100 (41.49) | |
| 2 | NA | 61 (25.31) | |
| 3 | NA | 39 (16.18) | |
| NR | NA | 3 (1.25) | |
-
*
Clinical information missing in eight retroperitoneal liposarcoma (RPLS) patients (training cohort 2).
-
†
The data is shown as mean (SD); other data is shown as number (%).
-
‡
The definition of surgical times is the sum of current admission surgery and previous surgical resection DDLS, dedifferentiated liposarcoma; LEP, leptin; MDM2, mouse double minute 2; MLS, myxoid liposarcoma; NA, not applicable; NR, not reported; PLS, pleomorphic liposarcoma; PTTG1, pituitary tumor transforming gene 1; WDLS, well-differentiated liposarcoma.
Cell cycle, DNA damage and repair, and metabolism are dysregulated in RPLS
To reveal the general molecular features of RPLS compared to noncancerous adipose tissues, we first recruited eight RPLS patients and collected paired tumor and normal tissues for DEG analysis. A total of 1354 DEGs, 554 upregulated and 800 downregulated, were identified (Figure 2A and B). To assess the underlying pathways of RPLS, GSEAs were performed for those DEGs. We found that proliferation-associated pathways, such as mitotic spindle, E2F target, G2/M checkpoint, and separation of sister chromatids, were mainly enriched in tumors, while metabolism-related pathways, such as bile acid metabolism, heme and fatty acid metabolism, and integration of energy metabolism, were enriched in normal controls (Figure 2C).
Figure 2
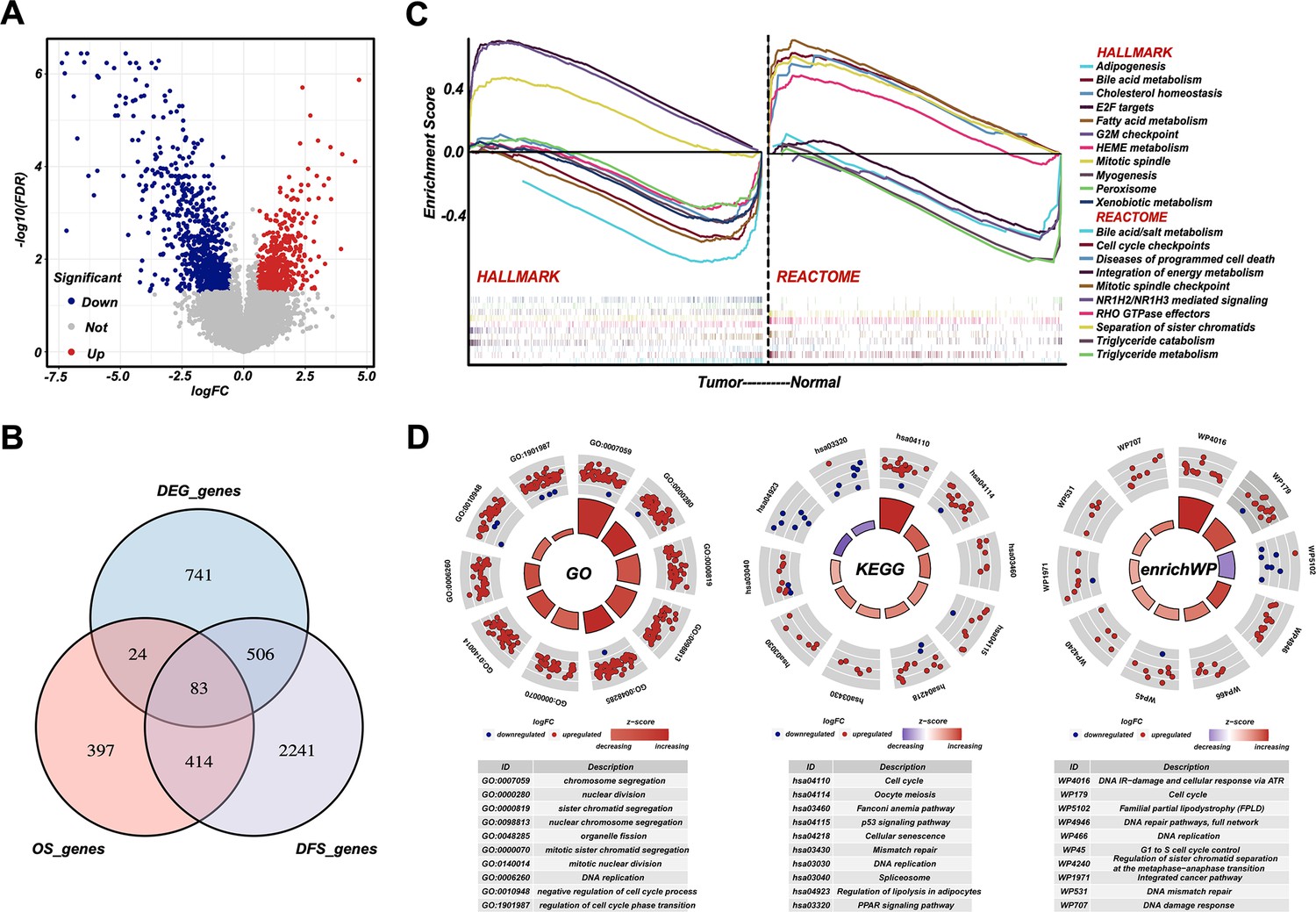
Cell cycle, DNA damage and repair, and metabolism are dysregulated in retroperitoneal liposarcoma (RPLS).
Volcano plot of the differentially expressed genes (DEGs) in eight normal vs eight RPLS tissues (A). Venn diagram showing shared genes between DEGs and prognostic genes (B). Gene set enrichment analysis (GSEA) of RPLS tumors, including HALLMARK gene sets and REACTOME gene sets (C). Circular plots of the prognostic genes in Gene Ontology (GO), Kyoto Encyclopedia of Gene and Genomes (KEGG), and enrichWP (D).
Then, we collected another 80 samples to investigate the molecular heterogeneity of RPLS. Gene expression profiles showed 918 and 3244 genes associated with OS and DFS, respectively. Among 497 candidate genes associated with both OS and DFS, 83 of them also overlapped with DEGs (Figure 2B). Functional annotation (GO, KEGG, and enrichWP) demonstrated that cell cycle, DNA damage and repair, and metabolism-related pathways were significantly enriched (Figure 2D), suggesting these signaling pathways were dysregulated in RPLS.
RPLS subgroups based on molecular features show different clinical outcomes
To evaluate heterogeneous molecular clustering characteristics in RPLS, ssGSEA emerged as a widely adopted method for computing the enrichment level of specific biological signaling pathways for each sample based on gene expression data. This aids in gaining insights into the overall activity level of signaling pathways. Here, we scored each sample on the dysregulated pathways by ssGSEA and divided RPLS patients into two subgroups (Figure 3A). Subgroup 1 (G1) showed better OS and DFS compared to subgroup 2 (G2) (Figure 3B and C). G1 displayed elevated ssGSEA scores associated with metabolism, whereas G2 exhibited heightened ssGSEA scores linked to cell cycle and DNA damage and repair (Figure 3D). These features suggested that effective monitoring of the prognosis of RPLS patients can be achieved based on the activation status of specific pathways. We also evaluated the clinical features and immune infiltration levels of those samples. The results showed that G1 had a lower aggressive pathological composition ratio, MDM2 and Ki67 expression, larger tumor size, and higher tumor microenvironment (TME) level compared to G2 (Figure 3E, G, H; Figure 3—figure supplement 1A and B). Surgery times for G1 were also tended to decrease (Figure 3F). Taken together, the above results indicated that RPLS subgroups based on molecular features showed distinct clinical features and clinical outcomes.
Figure 3 with 1 supplement see all
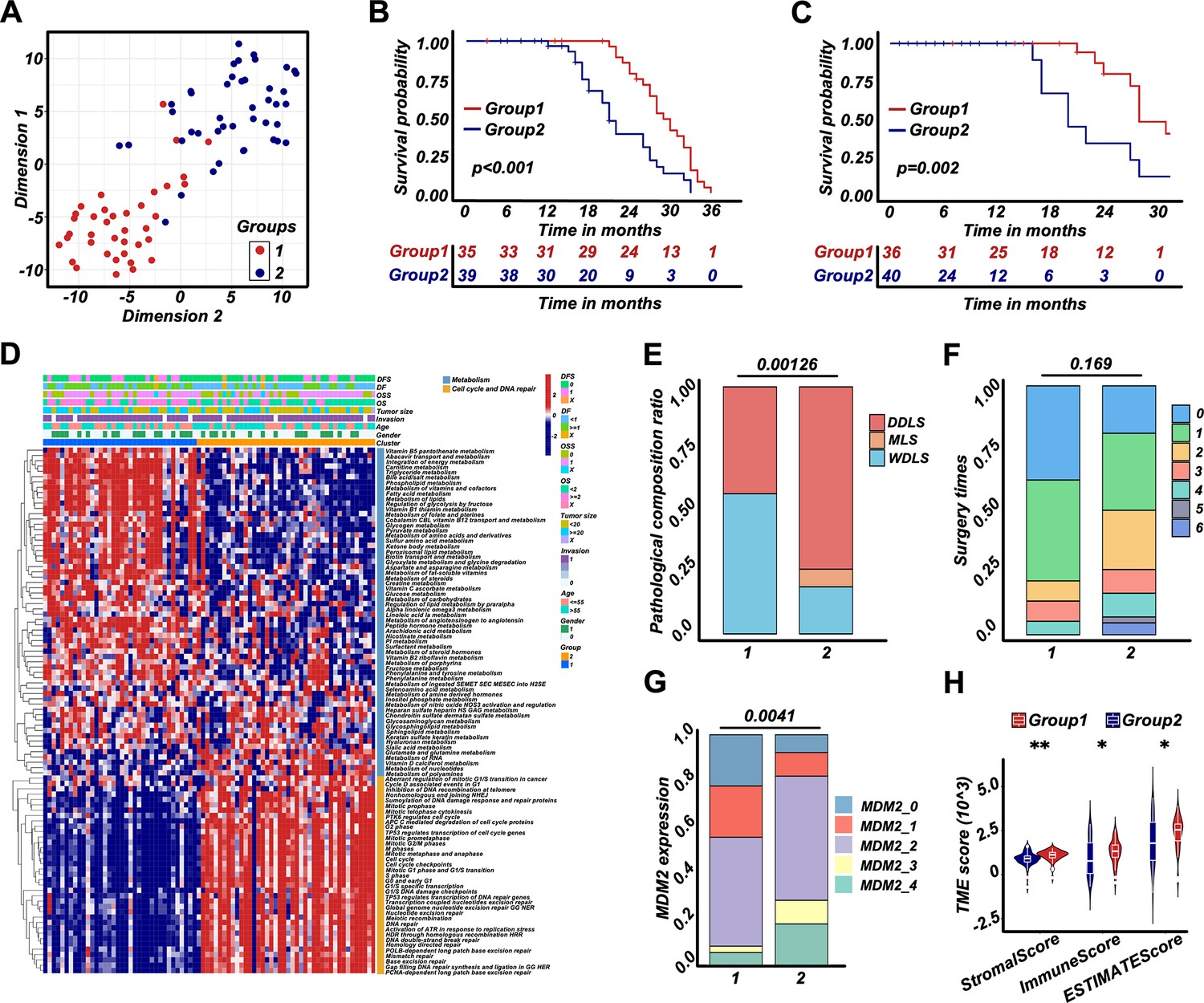
Retroperitoneal liposarcoma (RPLS) subgroups (G1 and G2) based on cell cycle, DNA damage and repair, and metabolism.
t-Distributed stochastic neighbor embedding (t-SNE) exhibited the subgroups (G1 and G2) of RPLS (A). Survival cures of overall survival (OS) (B) and disease-free survival (DFS) (C) in G1 and G2. The hierarchical clustering heatmap of dysregulated pathways in G1 and G2 (D). Histograms revealed the difference in pathological composition ratio (E), surgery times (F), and MDM2 (G) in G1 and G2. Violin plot of the microenvironmental scores in G1 and G2 (H).
A simplified RPLS classification strategy derived from RPLS G1/G2 subgroups
To explore representative biomarkers for different RPLS subgroups, we performed a DEG analysis between G1 and G2. There were 1258 genes downregulated, among which 112 of them indicated good prognosis (protective genes). Correspondingly, 754 genes were upregulated, and 28 of them indicated poor prognosis (aggressive genes) (Figure 3—figure supplement 1C and D). Enrichment analysis suggested that those DEGs were also associated with cell cycle regulation and metabolism (Figure 3—figure supplement 1E), which was consistent with previous results (Figure 2C).
To develop a simplified RPLS clustering based on DEGs, we adopted NMF and t-SNE for a reclassification of those patients. The results showed RPLS patients were also divided into two clusters (Figure 4A and Figure 3—figure supplement 1F and G). We then annotated the samples of two clusters by ssGSEA and found Cluster1 (C1) was related to metabolic processes, and Cluster2 (C2) was mainly related to the processes of cell cycle and DNA damage and repair (Figure 4—figure supplement 1A). Also, C1 showed better OS and DFS, lower pathological composition ratio and MDM2 expression, and fewer surgery times (Figure 4B–F). Lower Ki67 expression and larger tumor size were observed in C2 (Figure 4—figure supplement 1B and C). Interestingly, the biological annotations of the C1/C2 classification were greatly consistent with G1/G2. Therefore, a simplified RPLS classification strategy derived from RPLS subgroups was provisionally established.
Figure 4 with 1 supplement see all
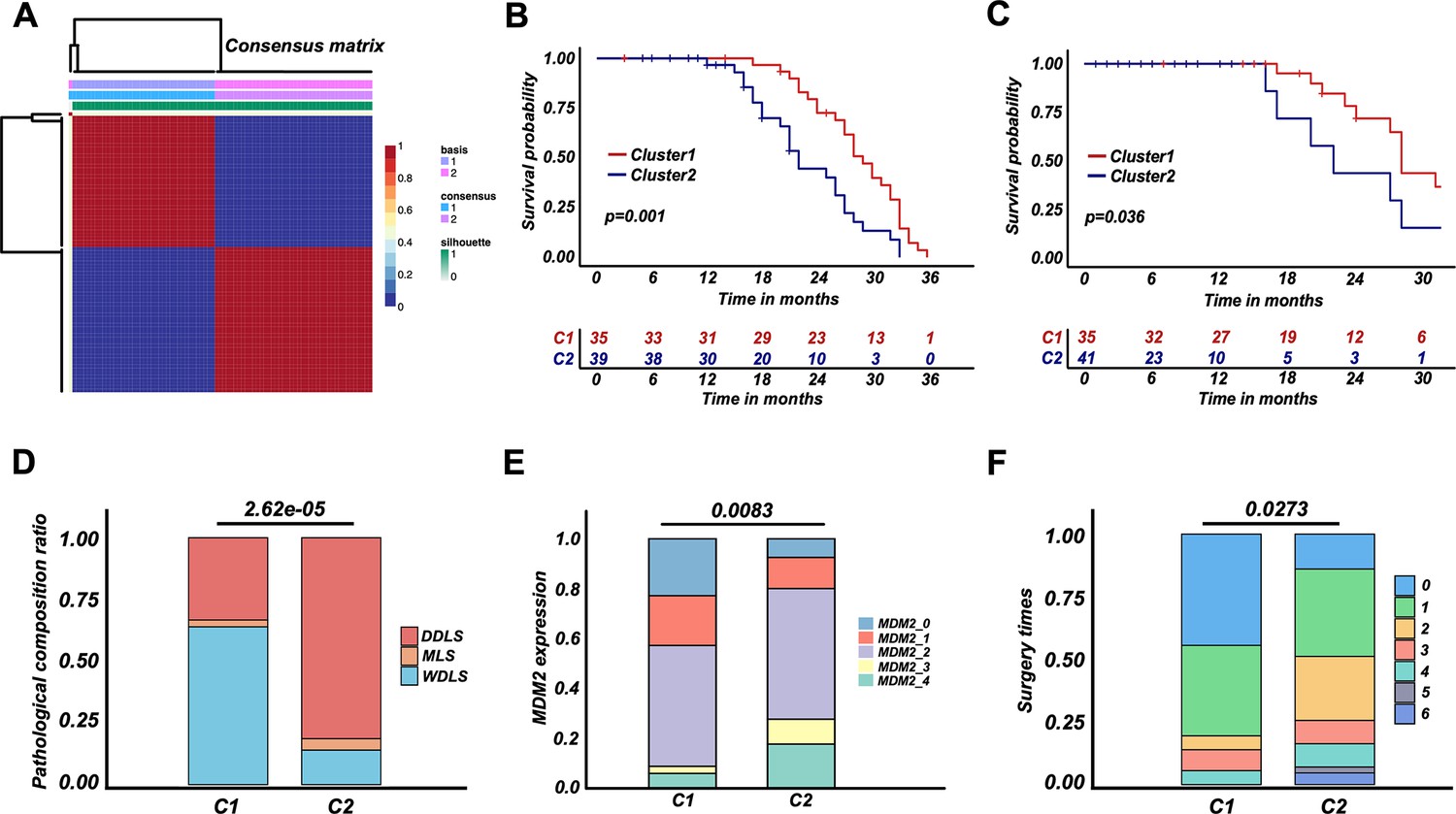
Retroperitoneal liposarcoma (RPLS) classification strategy (C1 and C2) derived from RPLS subgroups.
Nonnegative matrix factorization (NMF) for a reclassification of training cohort 1 (C1 and C2) (A). Survival cures of overall survival (OS) (B) and disease-free survival (DFS) (C) in C1 and C2. Histograms revealed the difference in pathological composition ratio (D), MDM2 (E), and surgery times (F) in C1 and C2.
Development of a dichotomous RPLS classification model
For NMF classification of RPLS patients, LEP and PTTG1 were identified as representative biomarkers of C1 and C2, respectively (Figure 5A). The selection criteria for identifying LEP and PTTG1 as biomarkers involved selecting prognostic genes that were highly expressed in C1 and C2, respectively, and achieved the highest AUC value in distinguishing the two RPLS groups. We aimed to replicate the RPLS classification of C1 and C2 by integrating these two biomarkers with the assistance of machine learning algorithms, and this two-gene panel achieved promising results (logistic, AUC = 0.995; SVM, AUC = 0.997; RF, AUC = 1.000; Figure 5B). Also, a linear negative correlation between LEP and PTTG1 expression was detected (Figure 5C). Considering the enhanced interpretability and generalization of linear models, we adopted the results of LR for subsequent analysis (risk values = 2.182 × PTTG1−2.204×LEP). The patients marked as high-risk (Cluster_H) exhibited worse OS and DFS than those marked as low-risk (Cluster_L) (Figure 5D and E). Dysregulated pathways, such as DNA repair and cell cycle regulation, were enriched in Cluster_H (Figure 5F; Figure 4—figure supplement 1D), and Cluster_H presented more aggressive pathological composition ratio, higher MDM2 levels, and marginally increased in surgery times than Cluster_L (Figure 5G–I). Similarly, the Cluster_H showed higher Ki67 levels and smaller tumor sizes (Figure 4—figure supplement 1E and F). Moreover, a Sankey diagram was drawn to show the correlation among G1/G2, C1/C2, and Cluster_L/H. Cluster_L/H was well matched to C1/C2 and G1/G2, suggesting LEP and PTTG1 were promising biomarkers for a dichotomous RPLS classification (Figure 5J). To ensure the broader applicability of LEP and PTTG1 as classification biomarkers, we performed an independent validation using an external liposarcoma cohort (GSE30929). This dataset was selected due to its relevance to RPLS (N=63, 45%) and the availability of distant recurrence-free survival (DRFS) outcomes, aligning with the clinical focus of our study. Applying our established LR, we found that the high-risk (V) group exhibited significantly worse DRFS compared to the low-risk (V) group (Figure 5—figure supplement 1A and B), and the high-risk group (V) demonstrated a higher proportion of high-grade histology (Figure 5—figure supplement 1C and D), consistent with our previous findings. These results validate the robustness and generalizability of our risk stratification model across distinct liposarcoma cohorts. The external dataset’s alignment with our findings underscores the potential of LEP and PTTG1 as reproducible biomarkers for prognosis and therapeutic stratification in liposarcoma.
Figure 5 with 1 supplement see all
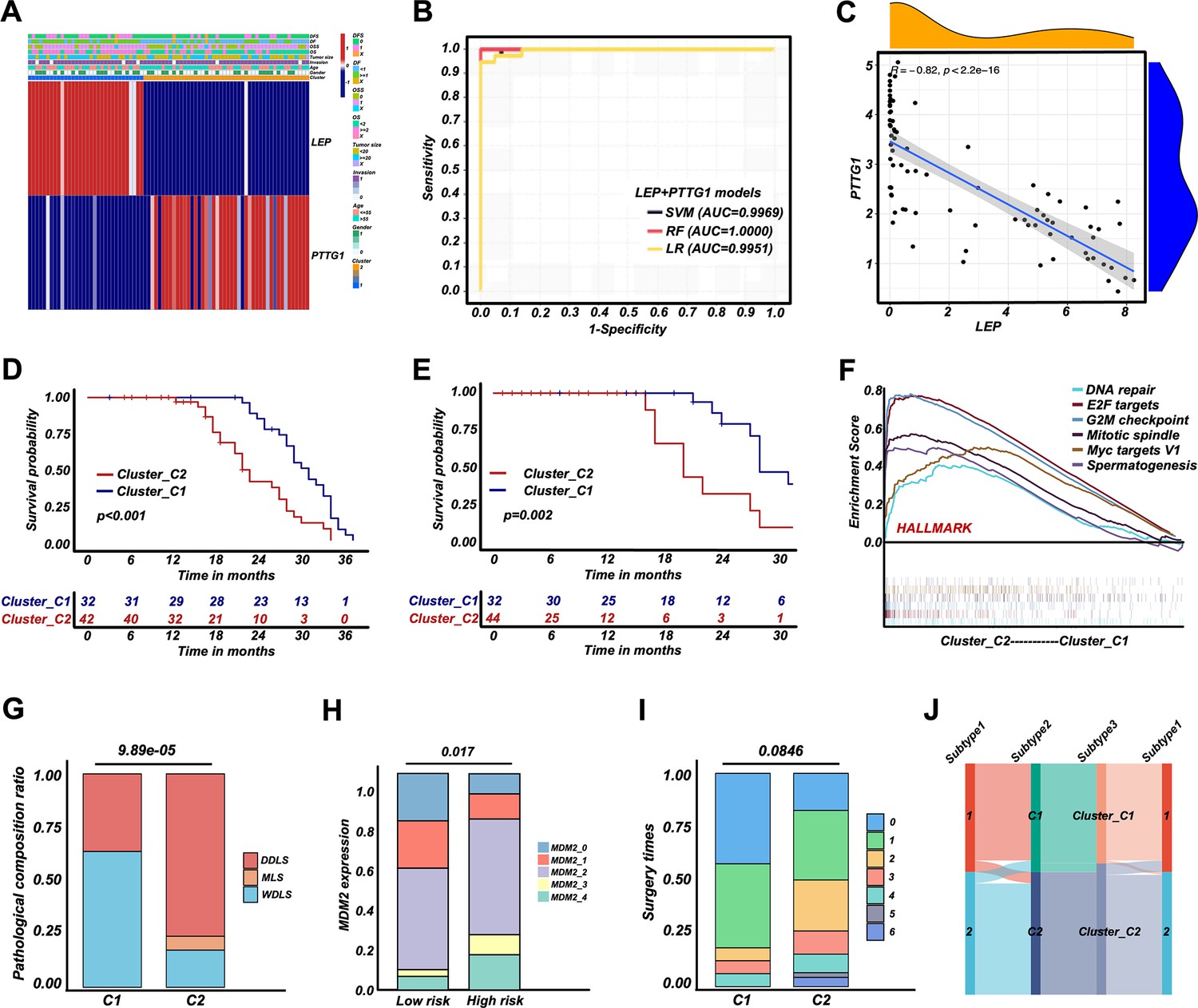
Retroperitoneal liposarcoma (RPLS) dichotomous classification (Cluster_C1 and Cluster_C2) derived from RPLS clusters.
Heatmap of biomarkers identified (LEP and PTTG1) in C1 and C2 (A). ROC curves of the machine learning models to identify C1 and C2 (B). Correlation between LEP and PTTG1 expression (C). Survival curves of overall survival (OS) (D) and disease-free survival (DFS) (E) in Cluster_C1 (low-risk) and Cluster_C2 (high-risk) groups. Gene set enrichment analysis (GSEA) of HALLMARK gene sets in Cluster_C1 and Cluster_C2 (F). Histograms revealed the difference in pathological composition ratio (G), MDM2 level (H), and surgery times (I) in Cluster_C1 and Cluster_C2. Sankey diagram indicated the correlation among G1/G2, C1/C2, and Cluster_C1/C2 (J).
Validation of the dichotomous RPLS classification in another 241 RPLS patients
To validate LEP and PTTG1 as biomarkers for a dichotomous RPLS classification, we performed IHC staining of two biomarkers in validation cohort. The representative images of LEP and PTTG1 with different expression levels were shown in Figure 6A and B. The IHC scores were integrated with the previously fitted coefficients to evaluate the prognosis of RPLS patients (risk values = 2.182×PTTG1IHC-2.204×LEPIHC). The cutoff value of validation cohort is the median of the risk value. The high-risk group had worse OS and DFS (Figure 6C and D), along with more surgery times and more aggressive pathological composition ratio (Figure 7A and B), but the difference in tumor size was not observed between the two groups (Figure 7C). Then, we constructed visual nomograms for a precise survival prediction of RPLS patients by combining the risk score with clinical features. The predictive abilities of the 1-, 2-, and 3-year OS (Figure 7D–F) and DFS (Figure 7—figure supplement 1A–C) were 0.743–0.788. Together, we proposed a simple and clinically applicable molecular classification strategy for RPLS patients.
Figure 6
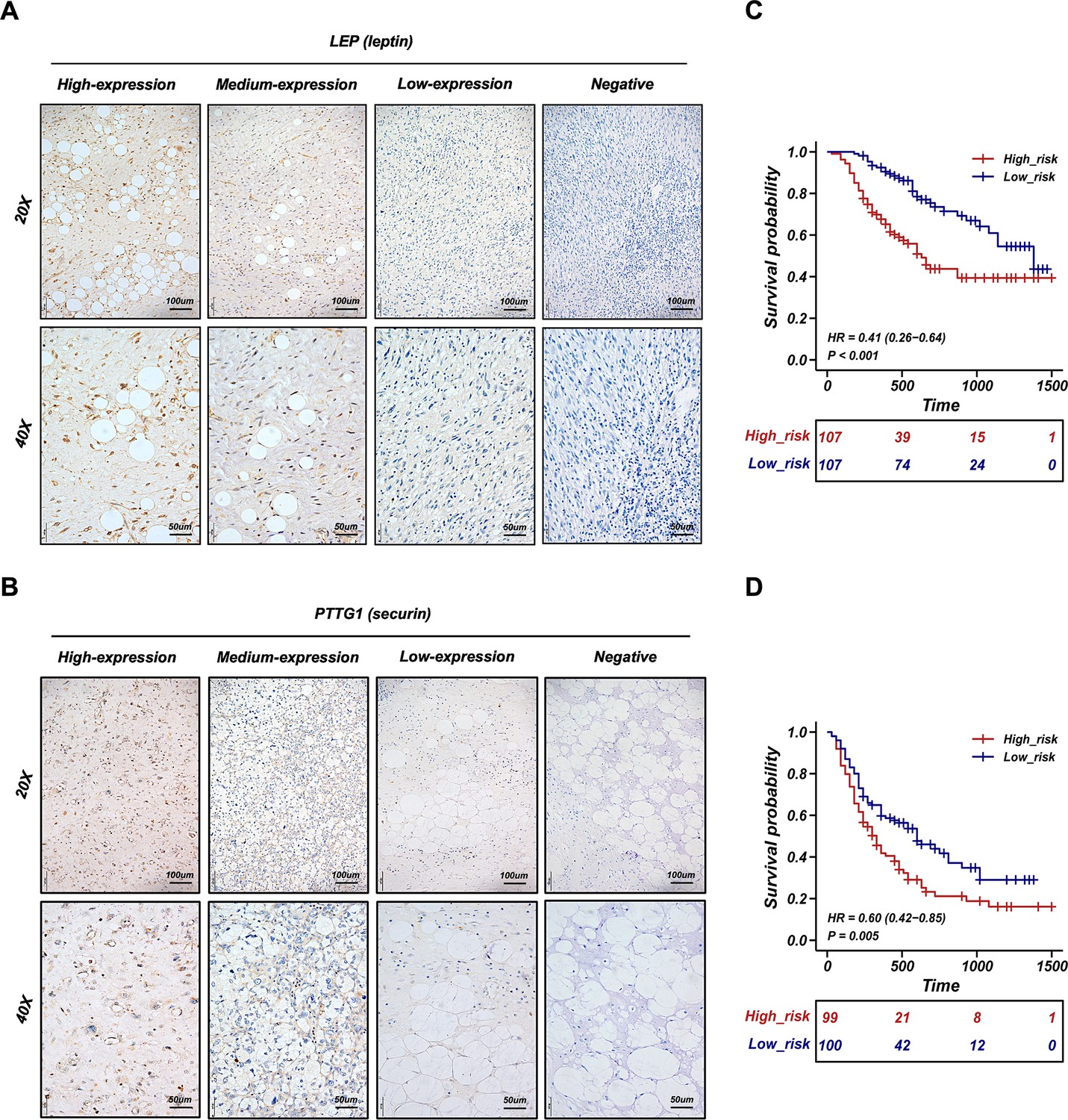
Validation of the retroperitoneal liposarcoma (RPLS) dichotomous classification in another 241 RPLS cohort.
Representative immunohistochemistry (IHC) staining images of LEP (A) and PTTG1 (B). Survival curves of overall survival (OS) (C) and disease-free survival (DFS) (D) in high-risk and low-risk groups.
Figure 7 with 1 supplement see all
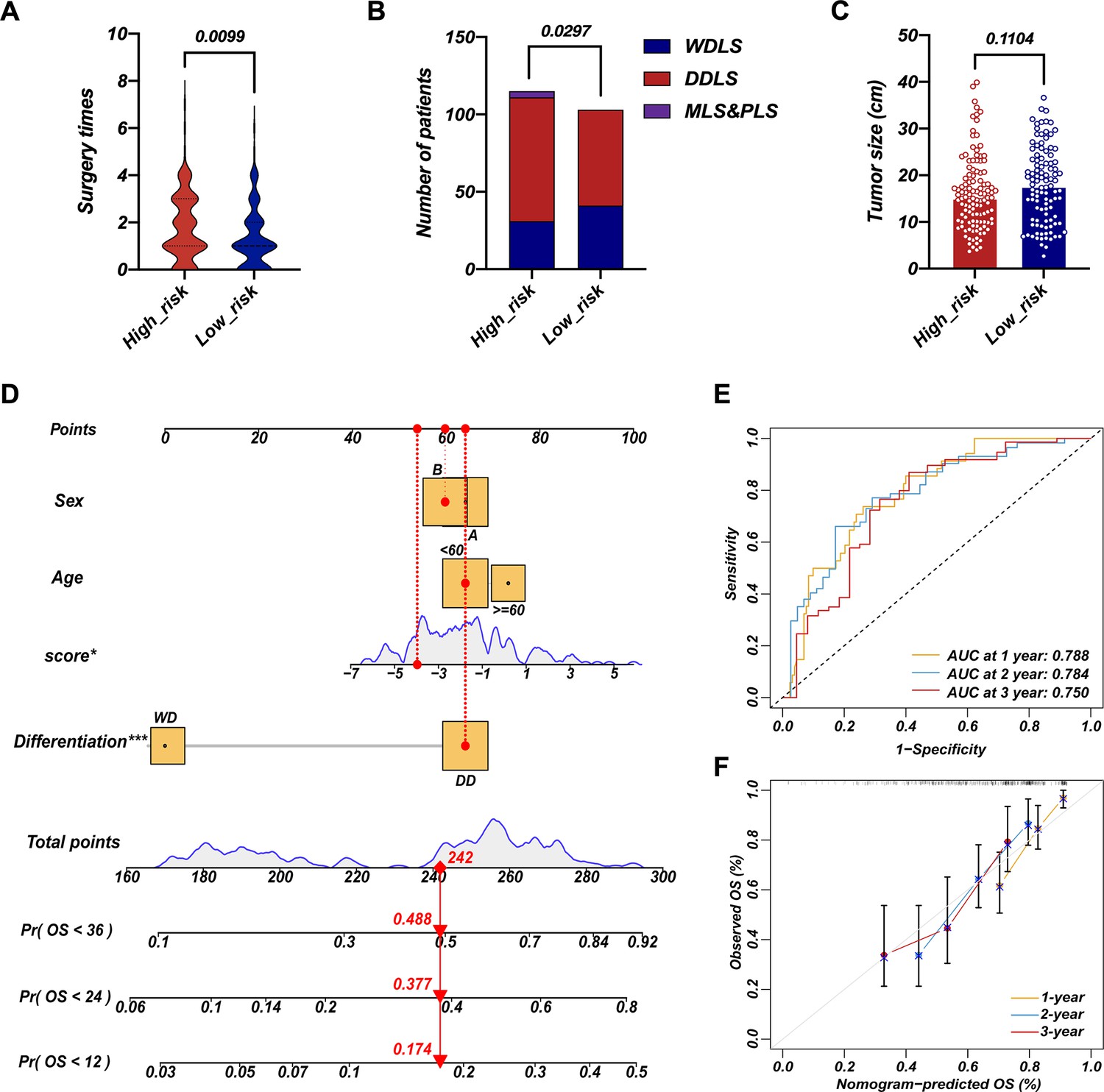
Survival nomogram of LEP+PTTG1 model in validation cohort.
The difference in surgery times (A), pathological composition (B), and surgery times (C) in high-risk and low-risk groups. Nomograms for overall survival (OS) were developed in REASR cohort with four factors: sex, age, risk score, and differentiation (D). ROC curves of 1-, 2-, and 3-year OS in validation cohort (E). Calibration curves of predicting 1-, 2-, and 3-year OS in validation cohort (F).
Discussion
Here, we divided RPLS patients into two subgroups based on cell cycle, DNA damage and repair, and metabolism-related pathways. G1 was annotated as metabolism-active, which exhibited high ssGSEA scores on metabolism-associated pathways, while G2 showed high ssGSEA scores on cell cycle and DNA damage and repair with a high Ki67 and MDM2 level.
G2 had more aggressive molecular features and worse clinical outcomes compared to G1, in accordance with previously reported tumor classification (Lindskrog et al., 2021; Yu et al., 2021; Zhang et al., 2022). In fact, the Cancer Genome Atlas Research Network. Electronic address: elizabeth.demicco@sinaihealthsystem.ca and Cancer Genome Atlas Research Network, 2017, has integrated SCNA and DNA methylation to divide dedifferentiated liposarcoma into two subtypes (S1 and S2), the unfavorable cluster was characterized as JUN amplified (an oncogene that promotes proliferation and metastasis) and lower inferred fraction of immature dendritic cells. However, the patients in the Cancer Genome Atlas Research Network. Electronic address: elizabeth.demicco@sinaihealthsystem.ca and Cancer Genome Atlas Research Network, 2017, were of complex origin (mixed limbs, trunk, and retroperitoneum), providing limited guidance for RPLS molecular classification. Here, we reported the first clinically applicable RPLS molecular classification based on RNA sequencing and IHC validation cohorts.
To facilitate the clinical application, we constructed a simplified RPLS molecular classification derived from the original cell cycle/metabolism subgroups. By the NMF algorithm, we identified LEP and PTTG1 as representative biomarkers for each subtype. A model based on IHC staining of LEP and PTTG1 successfully approximated the original dichotomous RPLS classification in biological features and survival outcomes. LEP is an important regulator of basal metabolism and food intake, which is considered a linkage between metabolism and the immune system (Jiménez-Cortegana et al., 2021). Although LEP-based targeting therapies have not yet been fully applied, LEP has already been identified as a potent metabolic reprogramming agent to support antitumor responses in aggressive melanomas (Waldman et al., 2020; de la Cruz-Merino et al., 2019; Rivadeneira et al., 2019). In addition, LEP improves the immunotherapeutic effects by regulating innate and adaptive immune responses via increasing the cytotoxicity of NK cells (Francisco et al., 2018), stimulating the proliferation of T/B cells (Francisco et al., 2018; Bernotiene et al., 2006), and activating DC cells (Hu et al., 2019). Those reported roles of LEP provided a good mechanism explanation on the features of metabolism pathway-enriched, better prognosis, and higher TME level of metabolism subgroup (LEP+). In contrast, PTTG1 acts as a regulator of sister chromatid separation during cell division under physiological conditions (Zou et al., 1999), which is closely linked to genetic instability, aneuploidy, tumor progression, invasion, and metastasis (Heaney et al., 2000; Ramaswamy et al., 2003; Kim et al., 2005; Yu et al., 2003; Teveroni et al., 2021; Romero et al., 2001). PTTG1 also regulates the cell cycle and the transactivation of growth factors as an initiator and promoter of tumorigenesis (Zou et al., 1999; Mora-Santos et al., 2013; McCabe et al., 2002; Ishikawa et al., 2001; Hamid et al., 2005). Overexpressing PTTG1 was correlated with worse prognosis in tumors, such as ovarian cancer (Parte et al., 2019), cervical cancer (Guo et al., 2019b), renal cell carcinoma (Tian et al., 2022), and colorectal cancer (Heaney et al., 2000). Therefore, the biological functions of PTTG1 provided a good mechanism explanation of the pathway-enriched cell cycle/DNA damage and repair-associated, worse prognosis, and more aggressive pathological composition ratio in the cell cycle subgroup (PTTG1+).
Conclusion
Our study presented a comprehensive gene expression landscape of RPLS, revealing distinct molecular features. Through categorizing RPLS into metabolism and cell cycle subtypes and identifying key biomarkers LEP and PTTG1, we established a dichotomous classification system verified by IHC assays. This innovative approach enables precise guidance for surgeons in adjusting treatment strategies for patients with histologically favorable but prognostically challenging RPLS cases, thereby advancing the implementation of precision medicine in guiding surgical interventions for RPLS.
Data anonymization
All participant identifiers were replaced with unique IDs during data collection and analysis.
Data availability
Data supporting the conclusions of this article are presented within the article and its supplementary files. Source data of Figure 2–5, Figure 3—figure supplement 1 and Figure 4—figure supplement 1 are available in Supplementary files 1, 2 and 4. Source data of Figure 6–7 and Figure 7—figure supplement 1 are available in Supplementary files 3. Source data of Figure 5—figure supplement 1 is available in GSE30929. The sequencing data (Supplementary files 1–4) of retroperitoneal liposarcoma have been deposited at the Open Archive for Miscellaneous Data (OMIX) database of China National Center for Bioinformation (CNCB) under the accession number OMIX002786. The data of the external validation cohort (GSE30929) was downloaded from GEO (https://www.ncbi.nlm.nih.gov/geo/). This paper does not report the original code.
-
CNCBID OMIX002786. Whole genome sequencing of retroperitoneal liposarcoma.
-
NCBI Gene Expression OmnibusID GSE30929. Whole-transcript expression data for liposarcoma.
-
CNCBID PRJCA014351. Whole genome sequencing of retroperitoneal liposarcoma.
References
-
Molecular and histopathology directed therapy for advanced bladder cancerNature Reviews. Urology 16:465–483.https://doi.org/10.1038/s41585-019-0208-0
-
The role of leptin in innate and adaptive immune responsesArthritis Research & Therapy 8:e2004.https://doi.org/10.1186/ar2004
-
MDM2 and CDK4 immunostainings are useful adjuncts in diagnosing well-differentiated and dedifferentiated liposarcoma subtypes: a comparative analysis of 559 soft tissue neoplasms with genetic dataThe American Journal of Surgical Pathology 29:1340–1347.https://doi.org/10.1097/01.pas.0000170343.09562.39
-
New horizons in breast cancer: the promise of immunotherapyClinical & Translational Oncology 21:117–125.https://doi.org/10.1007/s12094-018-1907-3
-
Preoperative radiotherapy in the management of retroperitoneal liposarcomaThe British Journal of Surgery 103:1839–1846.https://doi.org/10.1002/bjs.10305
-
Obesity, fat mass and immune system: role for leptinFrontiers in Physiology 9:640.https://doi.org/10.3389/fphys.2018.00640
-
A high-risk luminal A dominant breast cancer subtype with increased mobilityBreast Cancer Research and Treatment 175:459–472.https://doi.org/10.1007/s10549-019-05135-w
-
Human pituitary tumor-transforming gene induces angiogenesisThe Journal of Clinical Endocrinology and Metabolism 86:867–874.https://doi.org/10.1210/jcem.86.2.7184
-
Current and emerging therapies for advanced biliary tract cancersThe Lancet. Gastroenterology & Hepatology 6:956–969.https://doi.org/10.1016/S2468-1253(21)00171-0
-
The Janus-faced role of TRPM2-S in retroperitoneal liposarcoma via increasing ROS levelsCell Communication and Signaling 20:128.https://doi.org/10.1186/s12964-022-00873-9
-
The importance of the margin of resection and radiotherapy in retroperitoneal liposarcomaAmerican Journal of Surgery 221:554–560.https://doi.org/10.1016/j.amjsurg.2020.11.041
-
Vascular endothelial growth factor, its receptor KDR/Flk-1, and pituitary tumor transforming gene in pituitary tumorsThe Journal of Clinical Endocrinology and Metabolism 87:4238–4244.https://doi.org/10.1210/jc.2002-020309
-
REporting recommendations for tumour MARKer prognostic studies (REMARK)British Journal of Cancer 93:387–391.https://doi.org/10.1038/sj.bjc.6602678
-
A single mutation in Securin induces chromosomal instability and enhances cell invasionEuropean Journal of Cancer 49:500–510.https://doi.org/10.1016/j.ejca.2012.06.024
-
PTTG1: a unique regulator of stem/cancer stem cells in the ovary and ovarian cancerStem Cell Reviews and Reports 15:866–879.https://doi.org/10.1007/s12015-019-09911-5
-
A molecular signature of metastasis in primary solid tumorsNature Genetics 33:49–54.https://doi.org/10.1038/ng1060
-
A guide to cancer immunotherapy: from T cell basic science to clinical practiceNature Reviews. Immunology 20:651–668.https://doi.org/10.1038/s41577-020-0306-5
-
Expression profile‑driven discovery of AURKA as a treatment target for liposarcomaInternational Journal of Oncology 55:938–948.https://doi.org/10.3892/ijo.2019.4861
-
Molecular pathogenesis, targeted therapies, and future perspectives for gastric cancerSeminars in Cancer Biology 86:566–582.https://doi.org/10.1016/j.semcancer.2021.12.004
Article and author information
Author details
Funding
Beijing Municipal Science and Technology Commission, Adminitrative Commission of Zhongguancun Science Park (Z191100006619081)
- Li Min
National Natural Science Foundation of China (82073390)
- Li Min
Young Elite Scientists Sponsorship Program (2023QNRC001)
- Mengmeng Xiao
The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
Acknowledgements
This work was supported by grants from the Beijing Municipal Science and Technology Project (Z191100006619081), National Natural Science Foundation of China (82073390), and Young Elite Scientists Sponsorship Program (2023QNRC001). The study sponsors had no role in the design and preparation of this manuscript.
Ethics
Clinical trial registration Unique identifying number or registration ID: NCT03838718.
Specimens of RPLS were obtained from Peking University International Hospital. The study protocol was approved by the Ethics Committee of Peking University International Hospital, Peking University Health Science Center (WA2020RW29) and conducted in accordance with Helsinki Declaration. All patients signed the informed consent.
Version history
- Sent for peer review:
- Preprint posted:
- Reviewed Preprint version 1:
- Reviewed Preprint version 2:
- Version of Record published:
Cite all versions
You can cite all versions using the DOI https://doi.org/10.7554/eLife.100887. This DOI represents all versions, and will always resolve to the latest one.
Copyright
© 2025, Xiao, Li, Bu et al.
This article is distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use and redistribution provided that the original author and source are credited.
Metrics
-
- 834
- views
-
- 62
- downloads
-
- 0
- citations
Views, downloads and citations are aggregated across all versions of this paper published by eLife.
Download links
A two-part list of links to download the article, or parts of the article, in various formats.
Downloads (link to download the article as PDF)
Open citations (links to open the citations from this article in various online reference manager services)
Cite this article (links to download the citations from this article in formats compatible with various reference manager tools)
Molecular feature-based classification of retroperitoneal liposarcoma: a prospective cohort study
eLife 14:RP100887.
https://doi.org/10.7554/eLife.100887.3




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}