Osteonecrosis in Gaucher disease in the era of multiple therapies: Biomarker set for risk stratification from a tertiary referral center
- Department of Internal Medicine, Yale University, United States
- Department of ENT, Head and Neck Surgery, Guilan University of Medical Sciences, Islamic Republic of Iran
- Department of Rheumatology, University of Toronto, Canada
- Department of Computer and Information Science, University of Massachusetts Dartmouth, United States
- Department of Radiology and Biomedical Imaging, Yale University, United States
- Translational Sciences, Sanofi, United States
Abstract
Background:
A salutary effect of treatments for Gaucher disease (GD) has been a reduction in the incidence of avascular osteonecrosis (AVN). However, there are reports of AVN in patients receiving enzyme replacement therapy (ERT) , and it is not known whether it is related to individual treatments, GBA genotypes, phenotypes, biomarkers of residual disease activity, or anti-drug antibodies. Prompted by development of AVN in several patients receiving ERT, we aimed to delineate the determinants of AVN in patients receiving ERT or eliglustat substrate reduction therapy (SRT) during 20 years in a tertiary referral center.
Methods:
Longitudinal follow-ups of 155 GD patients between 2001 and 2021 were analyzed for episodes of AVN on therapy, type of therapy, GBA1 genotype, spleen status, biomarkers, and other disease indicators. We applied mixed-effects logistic model to delineate the independent correlates of AVN while receiving treatment.
Results:
The patients received cumulative 1382 years of treatment. There were 16 episodes of AVN in 14 patients, with two episodes, each occurring in two patients. Heteroallelic p.Asn409Ser GD1 patients were 10 times (95% CI, 1.5–67.2) more likely than p.Asn409Ser homozygous patients to develop osteonecrosis during treatment. History of AVN prior to treatment initiation was associated with 4.8-fold increased risk of AVN on treatment (95% CI, 1.5–15.2). The risk of AVN among patients receiving velaglucerase ERT was 4.68 times higher compared to patients receiving imiglucerase ERT (95% CI, 1.67–13). No patient receiving eliglustat SRT suffered AVN. There was a significant correlation between GlcSph levels and AVN. Together, these biomarkers reliably predicted risk of AVN during therapy (ROC AUC 0.894, p<0.001).
Conclusions:
There is a low, but significant risk of AVN in GD in the era of ERT/SRT. We found that increased risk of AVN was related to GBA genotype, history of AVN prior to treatment initiation, residual serum GlcSph level, and the type of ERT. No patient receiving SRT developed AVN. These findings exemplify a new approach to biomarker applications in a rare inborn error of metabolism to evaluate clinical outcomes in comprehensively followed patients and will aid identification of GD patients at higher risk of AVN who will benefit from closer monitoring and treatment optimization.
Funding:
LSD Training Fellowship from Sanofi to MB.
Editor's evaluation
This study presents valuable findings on the risk factors of avascular osteonecrosis in patients with Gaucher disease. The evidence supporting the claims of the authors is convincing. The work will interest clinicians who treat patients with inborn errors of metabolism.
https://doi.org/10.7554/eLife.87537.sa0Introduction
In Gaucher disease (GD), biallelic mutations in GBA1 result in defective lysosomal glucocerebrosidase and the cellular accumulation of glucosylceramide (GlcCer) and its downstream metabolite, glucosylsphingosine (GlcSph) (Mistry et al., 2015; van Dussen et al., 2014). These lipids accumulate classically in tissue macrophages and trigger a cascade of myeloid cell activation and chronic metabolic inflammation (Orvisky et al., 2002; Rigante et al., 2017; Nair et al., 2015; Nair et al., 2016).
Classical disease manifestations of GD include hepatosplenomegaly, cytopenia, and complex skeletal disease involving marrow infiltration, bone pain, osteopenia, fragility fractures, and recurrent avascular osteonecrosis (AVN) (Hughes et al., 2019; Grabowski et al., 2019; Yeh et al., 2009). In the neuronopathic forms of the disease (GD type 2 and type 3), there is additionally childhood onset of neurodegeneration, spinal deformity, pectus carinatum, and pulmonary involvement. Remarkably, severely disabling skeletal manifestations, would a priori, will be expected to be associated with commensurate severe involvement of other disease compartment, but no such relationship can be discerned (Khan et al., 2012). In a large study from the International Gaucher Registry (ICGG, ClinicalTrials.gov: NCT00358943), occurrence of AVN did not correlate with severity of hepatosplenomegaly, genotype, thrombocytopenia, or extent of elevation of the disease biomarker, chitotriosidase. Only low hemoglobin and previous splenectomy were correlated with risk of AVN (Khan et al., 2012). Therefore, clinicians and patients must remain vigilant of risk of AVN whether or not receiving treatment. Fortunately, there has been a reduction in the incidence of AVN since enzyme replacement therapy (ERT) with macrophage mannose receptor (MMR)-targeted imiglucerase became the standard of care in 1990s (Mistry et al., 2009b). The incidence of osteonecrosis in untreated GD patients was reported to be 22.8 per 1000 person years (95% CI, 20.2–25.7) of follow-up. In small single center studies, AVN was reported in as many as half of GD patients (Desnick et al., 1981; Deegan et al., 2011). The introduction of ERT in the 1990s led to reduction in the incidence of AVN to 13.8 per 1000 years of follow-up. Studies have also shown striking reduction in reports of bone pain and bone crisis in the era of therapeutics (van Dussen et al., 2014; Mistry et al., 2017). Since 2010, two other MMR-targeted ERTs have become available: velaglucerase and taliglucerase (Cox, 2013; Zimran et al., 2013; Gonzalez et al., 2013). Specific impact of newer ERTs on risk of AVN is not known. A recent introduction to first-line therapies for GD1 includes substrate reduction therapy (SRT), using eliglustat, a potent inhibitor of GlcCer synthase. In the extensive clinical trial program spanning more than 10 years, only few episodes of AVN were reported (Cox et al., 2023). In the placebo-controlled ENGAGE trial, there was only one case of AVN, which occurred in a patient receiving placebo (Mistry et al., 2021).
Despite the success of ERT in reducing the risk of AVN, there are occasional reports of AVN occurring in patients receiving ERT (Goker-Alpan, 2011; Potnis et al., 2019; de Fost et al., 2008). Therefore, it becomes important to understand whether there are identifiable risk factors for AVN, despite receiving GD-specific therapy. Knowledge of such factors will guide physicians in more comprehensive monitoring of patients beyond hematological and visceral disease as well as potentially advance understanding of underlying mechanisms. Prompted by AVN occurring in two pediatric patients despite ERT, we conducted an analysis of longitudinally followed patients at our tertiary national referral center to identify risk factors for AVN among patients receiving GD-specific therapy. We found patients with compound heterozygous p.Asn409Ser/other genotype, compared to p.Asn409Ser homozygous genotype, were at higher risk of AVN. Other risk factors included history of prior AVN before treatment initiation, type of ERT, and serum level of GlcSph, a validated biomarker of GD. GlcSph is downstream metabolite produced by deacylation of GlcCer via acid ceramidase. GlcSph is a relevant biomarker to study inflammatory manifestations of GD including AVN, as it is known to trigger immune activation and osteoblast dysfunction (Nair et al., 2015; Dekker et al., 2011; Murugesan et al., 2016; Saville et al., 2020).
Methods
Patients
We conducted a retrospective study of 187 GD patients longitudinally followed from 2001 to December 2021 at our center. Our observational study is approved by Yale’s Human Investigation Committee. A total of 155 patients met the inclusion criteria including confirmed diagnosis of GD by enzymatic and molecular testing, known treatment status and date of initiation/switch (imiglucerase, velaglucerase, and eliglustat), known splenectomy status, previous history of AVN and longitudinal data of MRI volumetrics for liver and spleen, CBC, and biomarkers including GlcSph and chitotriosidase.
Diagnosis of GD was based on diminished levels (<10% compared to controls) of acid β-glucosidase activity in peripheral blood leukocytes and full GBA1 sequencing using a combination of pacBio sequencing, WES, and Sanger sequencing, as described previously (Drelichman et al., 2021). Patients were followed every 1–2 years with standard of care evaluations, including MRI to assess organomegaly and marrow infiltration, and laboratory testing (Charrow et al., 1998). Volumetric MRI of liver and spleen was converted to multiples of normal with normal liver volume: 2.5% of body weight and normal spleen volume: 0.2% body weight. Patients developing new bone pain were evaluated earlier. Serum samples were collected at each clinic visit to determine biomarker trends for GlcSph and chitotriosidase, as well as other indicators of disease activity.
Surrogate disease biomarkers
Serum chitotriosidase activities were determined using a method described previously, with slight modifications (Schoonhoven et al., 2007). Briefly, assay buffer was adjusted to pH 4.5, and the final concentration of 4- methylumbelliferyl-beta-D-N,N’,N”-triacetylchitotriose fluorogenic substrate was 10 µM. CHIT1 genotyping was performed to normalize serum levels as described previously (Boot et al., 1998). Serum GlcSph levels were measured via liquid chromatography coupled to tandem mass spectrometry (Murugesan et al., 2016). Normal healthy control levels were ≤1 ng/ml.
AVN episodes
Generally, episodes of AVN were associated with new bone pain or exacerbation of chronic bone pain that prompted new visits, earlier than regular 1–2 yearly follow-ups. Occasionally, we found new AVN on MRI scans and on closer questioning patients reported bone pain that they managed symptomatically.
Statistical analysis
Frequency and percentage were used to describe qualitative data and mean, and standard deviation were used for quantitative data. Mixed-effects logistic regression was applied to analyze repeated-measure data during treatment. In this study, three mixed-effects models were fitted on the data: a logistic mixed-effects model with the response of AVN incidence and two linear mixed models with the responses of chitotriosidase and GlcSph to different therapies. A random intercept was chosen to account for the presence of different quantitative variables and the uniformity of sizes with different numbers for patients (Detry and Ma, 2016). To compare the effect of each treatment on the changes of chitotriosidase and GlcSph, a linear mixed model with two-by-two Bonferroni comparisons was used. The structure of logistics mixed model was as follows:
where Yi is a binary variable describing the outcome of case i (0 or 1), β is a fixed parameter vector, xi is a covariate vector for fixed effects, u is a vector of random variables from probability distributions, and zi is a covariate vector for random effects. u represents unmeasured covariates as a way of modeling heterogeneity and correlated data.
In the model used in our study, the response variable is incidence of AVN during treatment (yes/no). For fixed effects, the covariates included type of treatment (imiglucerase, velaglucerase, and eliglustat), previous history of AVN (occurrence and non-occurrence), sex, GBA1 genotype, spleen status (intact spleen with volumetric measurement or splenectomized), and GlcSph, chitotriosidase, hemoglobin, platelet count, spleen volume, liver volume. The random effect was intercept. Several variance-covariance structures were examined for obtaining the best fit. To make this selection, Akaike’s information criteria was used for the least value. Autoregressive of Order 1 (Ar (1)) was chosen based on this criterion. All statistical analyses were performed with SPSS version 28 (SPSS Inc, Chicago, IL, USA). A p-value <0.05 was considered statistically significant. MedCalc version 20.026 was used for ROC curve analysis and graphs were plotted by GraphPad Prism version 9.3.1.
Illustrative cases: the importance of awareness of AVN in pediatric patients
Two illustrative cases underscore the premise for our study. Patient 1 was born in in 2006–2010, had presented at pre-school age with history of chronic epistaxis and easy bruising, and found to have cytopenia and splenomegaly. The proband was diagnosed with GD1, GBA1 genotype p.Asn409Ser/c.217delC mutations. Liver and spleen volumes were 1.68 and 10.68 multiples of normal respectively. The patient was commenced velaglucerase ERT at dose 60 U/kg/2 weeks. The patient developed infusion-associated reactions (IARs) initially controlled with premedication but became refractory by 24th infusion and was switched to taliglucerase ERT which also caused IARs. Further switch back to velaglucerase caused recurrent IARs. Hematological parameters began to decline and at age 6–10 and developed severe pain in femur concerning for AVN. Plain radiology was normal. Symptoms progressed, and patient was confined to the wheelchair. MRIs revealed diffuse bone marrow signal abnormality throughout the femur consistent with osteonecrosis in left femur (Figure 1A). Few months later, the patient developed AVN in right femur (Figure 1B). Patient was evaluated at our center 1 year later. The patient appeared chronically ill and in pain, was in wheelchair, and had limited ability to weight-bear. Further studies revealed that patient had developed pan-neutralizing antibodies to all enzyme preparations (velaglucerase, imiglucerase, taliglucerase) after starting velaglucerase ERT. Due to high risk of extension of primary AVN in the femora and recurrent AVN at other sites, we secured approval from our IRB for treatment with eliglustat via Emergency Use Protocol. During past 6 years on eliglustat, there have been no further bone crises, Hb increased from 10.6 to 13.6, and platelets from 107 to 184. Concomitantly, serum GlcSph was reduced from 644 ng/ml to 101 ng/ml.
Figure 1
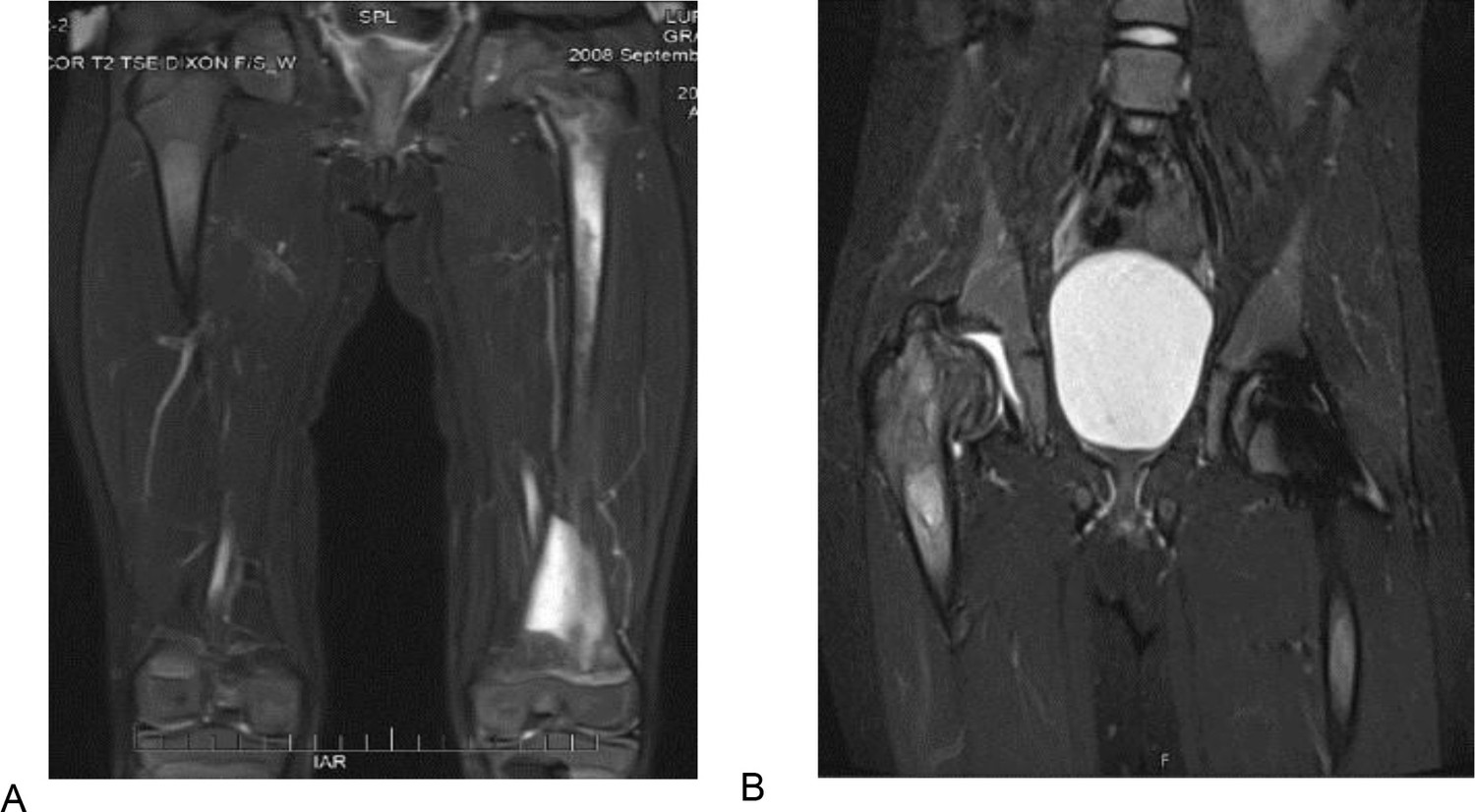
T2 weighted and STIR MR images of the patient 1 described in section Illustrative cases: the importance of awareness of AVN in pediatric patients.
(A) T2 weighted MR image of the femurs, showing diffuse bone marrow signal abnormality throughout the left femur with associated periostitis and subperiosteal fluid collection. (B) STIR MR image of the pelvis of the same patient 1 year after. (A) showing an expanding lesion of the greater trochanter, superiorly displacing fragments of bone and collapsed right hip joint.
Patient 2
The proband who was in good state of health, started to suffer from left femur pain during school age requiring multiple ER admissions. Initial diagnosis included leg sprain, growing pains, Lyme arthritis, and then osteomyelitis based on MRI findings. Despite antibiotics, femur pain persisted and pathology of debridement for presumed osteomyelitis was positive for Gaucher cells. GBA1 genotype was p.Asn409Ser/p.Leu483Pro mutations. The proband was started on velaglucerase ERT but few months later, the patient had recurrent AVN in left femur. The patient was switched to imiglucerase and has been remained free of AVN and hematological, visceral, and biomarkers indicators show stable GD activity. More recently after the patient turned young adult, was switched to eliglustat SRT and continued to do well.
Results
Patient demographics and AVN on treatment
The demographics of patients in the study are shown in Table 1. The cohort comprises 79 (50.3%) male individuals. Of the 155 patients studied, 42 (27.1%) had history of osteonecrosis prior to treatment initiation and 32 patients (20.6%) had undergone prior splenectomy.
Table 1
Demographic characteristics of the patients in this study.
Among 187 Gaucher disease patients followed longitudinally from 2001 to December 2021, a total of 155 patients met the inclusion criteria (explained in section Patients). Qualitative data were described by frequency and percentage and mean, and standard deviation (SD) were used for quantitative data. GBA1: glucosylceramidase beta 1, WBC: white blood cell, HgB: hemoglobin.
| All(N=155) | All(N=155) | ||
|---|---|---|---|
| Age at first visit (year) | Number of visits | ||
| Mean (SD) | 33.81 (18.74) | Mean (SD) | 6.1 (4.17) |
| Median (min, max) | 34 (2, 85) | Median (min, max) | 5.0 (1, 25) |
| Gender | Duration of follow-up (year) | ||
| Female:Male | 77 (49.7 %):78 (50.3%) | Mean (SD) | 14.0 (12) |
| Age at first symptoms (year) | Median (min, max) | 12(1,20) | |
| Mean (SD) | 20.02 (16.1) | Osteonecrosis while untreated | |
| Median (min, max) | 17.0 (5, 65) | Yes | 42 (27.1%) |
| Age at diagnosis (year) | No | 113 (72.9.%) | |
| Mean (SD) | 23.2 (17.3) | Spleen status | |
| Median (min, max) | 22.0 (5, 67) | Intact spleen | 123 (79.4%) |
| Gap to diagnosis in men (year) | Splenectomized | 32 (20.6%) | |
| Mean (SD) | 11.2 (12.6) | Type of treatment (year) | |
| Median (min, max) | 5.5 (0, 57) | Imiglucerase | 834 (60.3%) |
| Gap to diagnosis in women (year) | Eliglustat | 238 (17.2%) | |
| Mean (SD) | 10.3 (11.2) | Velaglucerase | 310 (22.4%) |
| median (min, max) | 7 (0, 40) | Clinical variables: mean (SD) | |
| Age at starting treatment (year) | Hermann score | 2.84 (1.6) | |
| Mean (SD) | 33 (18) | Severity score index | 7.62 (3.8) |
| Median (min, max) | 29 (2, 85) | Chitotriosidase (nmol/hr/ml) | 1106.15 (2801.3) |
| Gap to start treatment (year) | Glucosylsphingosine (ng/ml) | 58.12 (22.5) | |
| Mean (SD) | 10.5 (11) | Liver volume in cc | 1676.40 (186.4) |
| Median (min, max) | 9 (0, 57) | Liver multiples of normal | 0.94 (0.24) |
| GBA1 genotype | Spleen volume in cc | 480.9 (146.8) | |
| p.Asn409Ser/p.Asn409Ser | 78 (51%) | Spleen multiples of normal | 3.47 (2.95) |
| p.Asn409Ser/p.Leu483Pro | 20 (13.1%) | WBC ×103 u/l | 6.46 (3.48) |
| p.Asn409Ser/84GG | 14 (9.2%) | Hgb in g/dl | 13.92 (1.6) |
| p.Asn409Ser/IVS2+1 | 6 (3.9%) | Platelets ×103 u/l | 200.6 (87.1) |
| p.Asn409Ser/other | 27 (17.6%) | ||
| Other/other | 8 (5.2%) |
During 20 years’ span of this study, there were 16 episodes of AVN in 14 patients, with two episodes, each occurring in two patients. In aggregate, the patients received 1382 cumulative years of treatment. By treatment type, total treatment years for imiglucerase ERT was 834 years and a total of six episodes of AVN occurred on imiglucerase ERT, that is 0.72 AVN per 100 years imiglucerase. Patients received cumulative 310 years velaglucerase ERT and there were 10 episodes of AVN, that is 3.2 AVN per 100 years of velaglucerase ERT. Total treatment years for eliglustat SRT was 238 years and so far, there have been no episodes of AVN among patients receiving eliglustat SRT. The demographics of these 14 patients shown in Table 2.
Table 2
Demographics and clinical features of patients with osteonecrosis on treatment at the proximity to avascular osteonecrosis (AVN) occurrence.
Modes of presentation of AVN shown as ‘painful’ indicating new onset of bone pain prompting early evaluation and ‘silent’ discovered on routine annual MRI and in retrospect, further history indicated patients had exacerbation of chronic pain that they treated symptomatically. * age range: C (child: age <18), YA (young adult: age 18–40), MA (middle-aged adult: age 40–60), OA (older adult: age >60). Shown are GBA1 genotype, age at AVN, type of treatment, history of AVN prior to treatment, serum biomarkers, liver/spleen volumes, and interval between diagnosis and initiation of treatment.
| AVNoccurrence | Gender | Genotype in GBA1 | Age at AVN (category)* | Type of ERT | History of AVN | Age at Diagnosis (category)* | Gap to diagnosis (years) | Age at ERT initiation (category)* | Gap to ERT initiation(year) | Type of AVN | Location | Hemoglobin(gm/dl) | Platelet(×1000 u/l) | Liver multiples of normal | Spleen multiples of normal | Chitotriosidase (nmol/hr/ml) | GlcSph(ng/ml) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Patient no. 1 | M | p.Asn409Ser /84GG | MA | Velaglucerase | No | C | 1 | YA | 23 | Silent | Femur | 17.1 | 111 | 0.89 | 5.2 | 389.8 | 93.7 |
| 2 | Patient no. 2 | F | p.Asn409Ser /p.Ile442Thr | MA | Velaglucerase | Yes | C | 1 | YA | 11 | Painful | Femur | 15.6 | 252 | 0.93 | 1.8 | 743.5 | 158.3 |
| 3 | Patient no. 3 | M | p.Leu483Pro /p.Asn501Lys | OA | Velaglucerase | Yes | MA | 1 | OA | 25 | Silent | Femur | 14.0 | 313 | 0.80 | Splenectemized | 332.9 | 69.2 |
| 4 | Patient no. 4 | F | p.Asn409Ser /p.Leu483Pro | YA | Imiglucerase | No | C | 0.2 | C | 0.1 | Silent | Femur | 13.3 | 244 | 0.96 | 1.56 | 1962 | 89.8 |
| 5 | Patient no. 5 | F | p.Asn409Ser /p.Leu483Pro | C | Velaglucerase | Yes | C | 3 | C | 0.1 | Painful | Femur | 13.4 | 212 | 1.12 | 3.1 | 731.4 | 143.5 |
| 6 | Patient no. 6 | M | p.Asn409Ser /p.Asp166Glu | MA | Imiglucerase | Yes | MA | 5 | MA | 0.4 | Painful | Shoulder | 15.8 | 90 | 1.82 | 9.1 | 3.4 | 248.2 |
| 7 | Patient no. 7 | F | p.Asn409Ser /p.Arg502Ser | MA | Velaglucerase | No | YA | 10 | YA | 12 | Painful | Femur | 11.6 | 238 | 1.49 | 5.8 | 731 | 85 |
| 8 | Patient no. 7 | Second episode | OA | Imiglucerase | Yes | Painful | Hip | 12.5 | 235 | 1.41 | 5.4 | 733.6 | 145.7 | |||||
| 9 | Patient no. 8 | F | p.Asn409Ser /c.217delC | MA | Imiglucerase | Yes | YA | 0.1 | YA | 9 | Painful | Femur | 11.0 | 222 | 0.8 | Splenectemized | 523.4 | 61.9 |
| 10 | Patient no. 8 | Second episode | MA | Velaglucerase | Yes | Painful | Femur | 10.1 | 322 | 0.75 | 623.9 | 77.7 | ||||||
| 11 | Patient no. 9 | F | p.Asn409Ser /IVS2+1 | OA | Imiglucerase | Yes | C | 7 | YA | 23 | Painful | Hip | 13.3 | 474 | 0.73 | Splenectemized | 563.6 | 128.4 |
| 12 | Patient no. 10 | M | p.Asn409Ser /p.Leu483Pro | MA | Imiglucerase | Yes | YA | 4 | MA | 22 | Painful | Ankle | 16.7 | 299 | 0.88 | Splenectemized | 3123.4 | 223.8 |
| 13 | Patient no. 11 | M | p.Arg463Cys /p.255Tyr | MA | Velaglucerase | Yes | MA | 1 | MA | 5 | Painful | Hip | 14.5 | 253 | 0.91 | 1.6 | 1852.5 | 86.3 |
| 14 | Patient no. 12 | F | p.Asn409Ser /c.217delC | C | Velaglucerase | No | C | 3 | C | 1 | Painful | Femur | 11.5 | 124 | 1.38 | 7.7 | 4134.6 | 318.6 |
| 15 | Patient no. 13 | F | p.Asn409Ser /p.Asn409Ser | MA | Velaglucerase | No | YA | 0 | YA | 10 | Painful | Hand | 13.6 | 189 | 0.83 | 1.5 | 26.2 | 21.9 |
| 16 | Patient no. 14 | M | p.Asn409Ser /84GG | MA | Velaglucerase | Yes | C | 0 | YA | 12 | Painful | Navicular | 13.7 | 147 | 1.12 | 4.15 | 0 | 210.3 |
Delineating the determinants of AVN on treatment
Mixed-effects logistic regression was applied for analyzing repeated-measure data during treatment to decipher risk factors for developing AVN on treatment (Table 3). Heteroallelic p.Asn409Ser GD patients were 10 times (95% CI, 1.5–67.2, p=0.003) more likely than p.Asn409Ser homozygous patients to develop osteonecrosis during treatment. History of AVN prior to treatment initiation increased the risk of AVN by 4.8-fold while receiving a specific GD treatment (95% CI, 1.5–15.24, p=0.008). The risk of AVN among patients who had received velaglucerase ERT was 4.7 times higher compared to patients receiving imiglucerase ERT (95% CI, 1.67–13.07, p=0.003). No patient receiving eliglustat SRT suffered AVN. There was a significant correlation between residual GlcSph levels and AVN (95% CI, 1.004–1.02, p=0.004). For every 1 ng/ml increase in the level of GlcSph, there was estimated 1.2% increase in the risk of developing osteonecrosis during treatment. Level of serum GlcSph at first and second episode of AVN in two patients further underscores the role of GlcSph for risk prediction. As shown in Table 2, patient # 7 had developed first AVN when GlcSph was 85 ng/ml. The second episode of AVN when the serum level of GlcSph was 145.7 ng/ml. Similarly, patient # 8 developed AVN while the serum level of GlcSph was 61.9 ng/ml. The second episode of AVN when the serum level of GlcSph was 77.7 ng/ml.
Table 3
Output of mixed-effects modeling.
To determine the clinical context in which avascular osteonecrosis (AVN) occurs in Gaucher disease (GD) patients while receiving enzyme replacement therapy (ERT). Eliglustat substrate reduction therapy (SRT) was not included in the model as there were no episodes of AVN on patients receiving this therapy at the time of analysis. A random intercept was chosen to account for the presence of different quantitative variables and the uniformity of sizes with different numbers for patients. (Further explanation in sections Statistical analysis and Delineating the determinants of AVN on treatment.)
| Fixed coefficients | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model term* | Coefficient | Std. error | t | Sig. | 95% Confidence interval | Exp(coefficient) | 95% Confidence Interval for Exp(coefficient) | |||
| Lower | Upper | Lower | Upper | |||||||
| Intercept | –9.392 | 1.2846 | –7.311 | <0.001 | –11.913 | –6.872 | 8.337E-5 | 6.705E-6 | 0.001 | |
| Rx: velaglucerase | 1.543 | 0.5235 | 2.948 | 0.003 | 0.516 | 2.570 | 4.680 | 1.676 | 13.071 | |
| Rx: imiglucerase | 0† | . | . | . | . | . | . | . | . | |
| AVN pre-Rx: Yes | 1.568 | 0.5894 | 2.659 | 0.008 | 0.411 | 2.724 | 4.795 | 1.508 | 15.243 | |
| AVN pre-Rx: No | 0† | . | . | . | . | . | . | . | . | |
| Gender: female | 0.859 | 0.5298 | 1.620 | 0.105 | –0.181 | 1.898 | 2.360 | 0.834 | 6.673 | |
| Gender: male | 0† | . | . | . | . | . | . | . | . | |
| Spleen status: Splenectomized | 0.754 | 0.5851 | 1.288 | 0.198 | –0.394 | 1.902 | 2.125 | 0.674 | 6.697 | |
| Spleen status: intact | 0† | . | . | . | . | . | . | . | . | |
| Genotype: other/other | 1.903 | 1.3717 | 1.387 | 0.166 | –0.789 | 4.594 | 6.705 | 0.454 | 98.919 | |
| Genotype: p.Asn409Ser/other | 2.309 | 0.9685 | 2.384 | 0.017 | 0.409 | 4.209 | 10.063 | 1.505 | 67.297 | |
| Genotype: p.Asn409Ser/p.Asn409Ser | 0† | . | . | . | . | . | . | . | . | |
| Serum level of glucosylsphingosine (ng/ml) | 0.012 | 0.0040 | 2.880 | 0.004 | 0.004 | 0.020 | 1.012 | 1.004 | 1.020 | |
-
Probability distribution: BinomialLink function: Logit.
-
*
Target: occurrence of AVN during treatment.
-
†
This coefficient is set to zero because it is redundant.
Assessing the role of serum GlcSph levels for the risk of AVN
ROC curve analysis was done to estimate cut-offs for GlcSph levels to predict the risk of AVN in GD patients while receiving treatment. The ROC curve shows true positive rate (sensitivity) as a function of the false positive rate (100-specificity) for different cut-off points. We found the value of the area under the ROC curve at GlcSph serum level of 77.64 ng/ml to be 0.857 (Figure 2A), that is GlcSph level is a significant variable correlated with the incidence of AVN while receiving treatment.
Figure 2
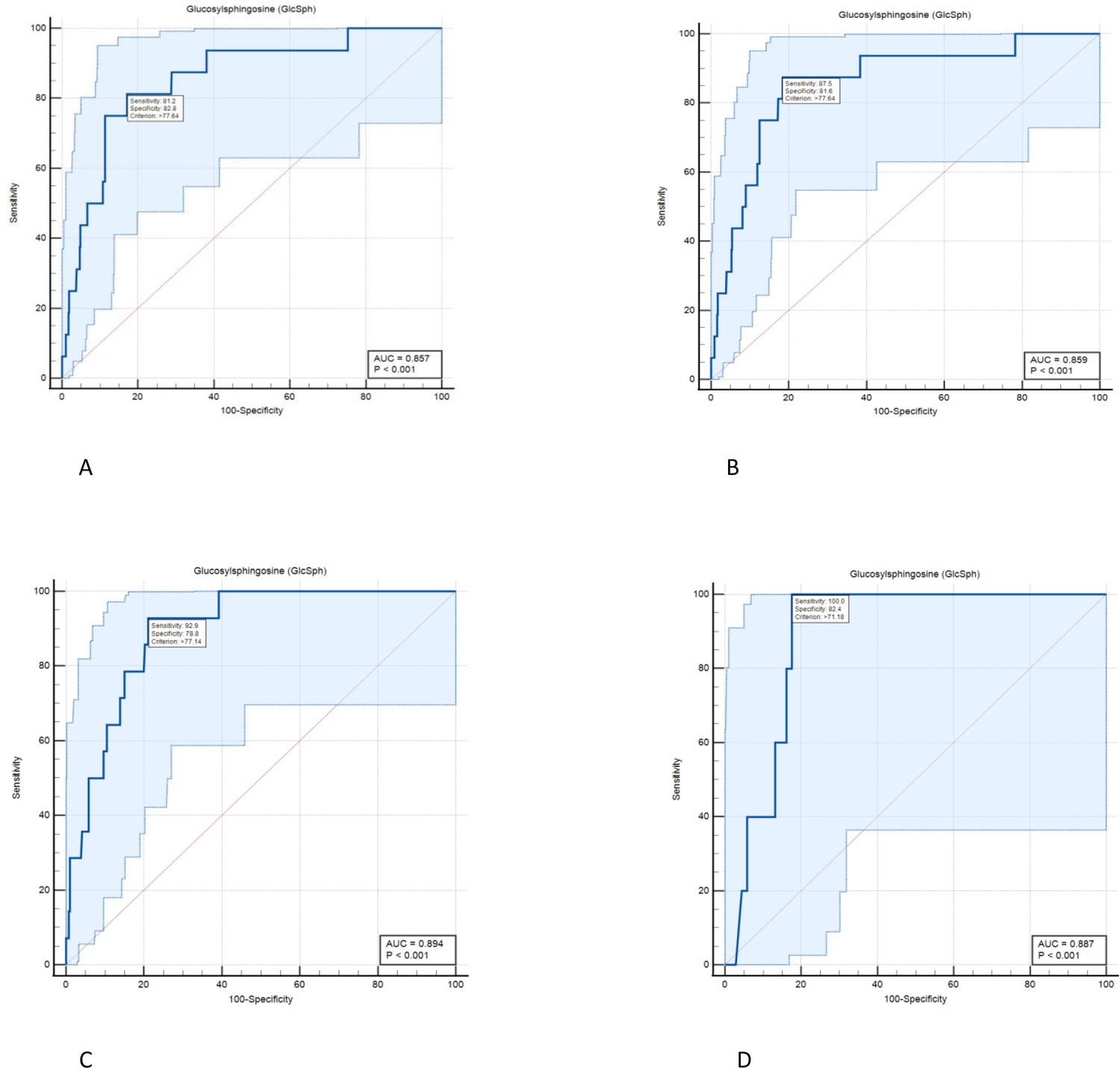
Diagnostic accuracy of serum level of glucosylsphingosine (GlcSph) for diagnosis of avascular osteonecrosis (AVN) on treatment: ROC curve analysis was done to assess the diagnostic accuracy cut-offs for GlcSph levels to predict the risk of AVN in Gaucher disease (GD) patients while receiving treatment.
(A) We found the value of the area under the ROC curve at GlcSph serum level of 77.64 ng/ml to be 0.857. GlcSph level of 77.64 ng/ml has sensitivity of 81.2% (95% CI, 54.4–96%) and specificity of 82.8% (95% CI, 80.7–84.8%) for association with AVN in entire GD patients receiving treatment. (B) As shown here, clinical significance of GlcSph levels is enhanced by considering their context of use regarding other risk factors. In patients with at least one of delineated risk factors in our study, that is compound heterozygosity for p.Asn409Ser, history of AVN prior to treatment or velaglucerase ERT, sensitivity for GlcSph level at 77.64 ng/ml increases to 87.5%. (C) In patients who harbor at least two of delineated risk factors in this study, GlcSph level of 77.14 ng/ml has sensitivity of 92.9% and specificity of 78.8% to rule in the probability of AVN on ERT. (D) In patients with all three risk factors delineated in the study, GlcSph level of 71.8 ng/ml is 100% sensitive to support the probability of AVN with specificity of 82.4%.
Effect of GD-specific therapies on biomarkers, Chitotriosidase and GlcSph
The three drugs used to treat GD showed differential response in reducing serum chitotriosidase activity. Velaglucerase appeared to be most effective in reducing chitotriosidase, followed by imiglucerase. Pairwise comparisons showed the mean chitotriosidase in patients receiving velaglucerase was significantly lower than eliglustat, however, no significant difference was observed between velaglucerase and imiglucerase (p>0.999), (Figure 3A).
Figure 3
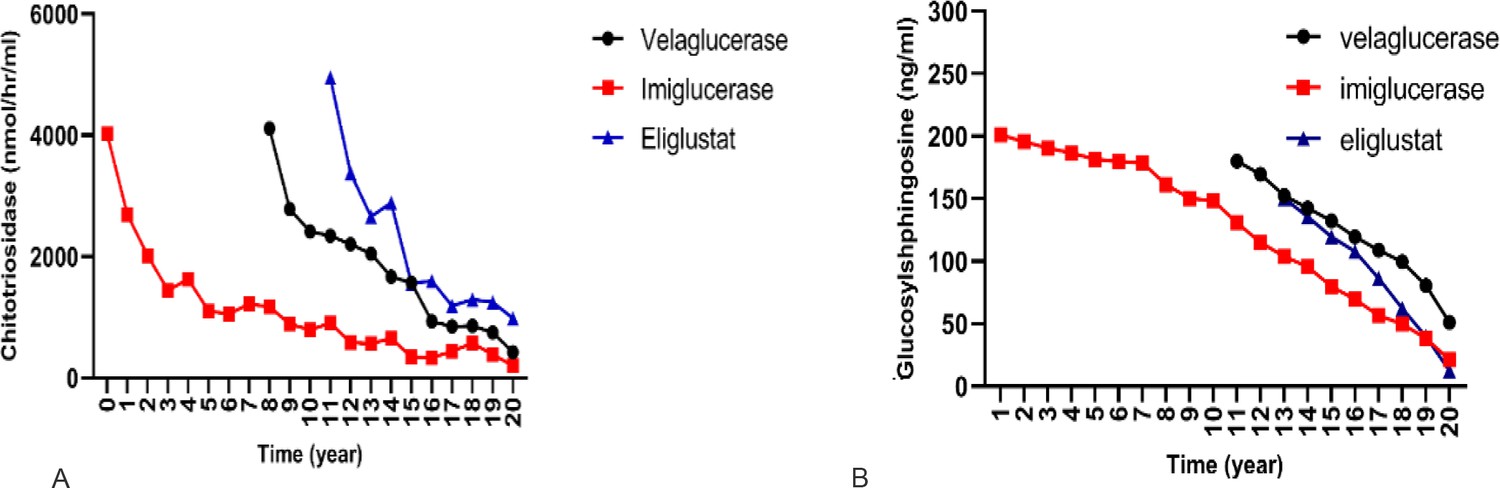
Effect of different therapies on chitotriosidase and glucosylsphingosine (GlcSph).
To compare the effect of each treatment on the changes of chitotriosidase and GlcSph, a linear mixed model with two-by-two Bonferroni comparisons was used.
(A) Effects of three drugs on chitotriosidase (nmol/hr/ml): pairwise comparisons showed velaglucerase is most effective in reducing chitotriosidase, followed by imiglucerase, followed by eliglustat. (B) Effects of three drugs on GlcSph (ng/ml): three drugs were significantly different for effect on GlcSph reduction (p<0.001). Eliglustat was the most effective in reducing serum GlcSph, followed by imiglucerase, followed by velaglucerase. Pairwise comparisons showed that the mean serum GlcSph in eliglustat-treated patients was significantly lower than the enzyme replacement therapies (ERTs). There was no significant difference in patients receiving velaglucerase vs imiglucerase (p=0.478).
Next, we examined serum GlcSph biomarker, and we found the three drugs were significantly different for effect on GlcSph reduction (p<0.001). Eliglustat was the most effective in reducing serum GlcSph, followed by imiglucerase, followed by velaglucerase. Pairwise comparisons showed that the mean serum GlcSph in eliglustat-treated patients was significantly lower than the ERTs. There was no significant difference in patients receiving velaglucerase vs imiglucerase (p=0.478). (Figure 3B).
Discussion
AVN is one of the most devastating and life-altering manifestations of GD that results in chronic disability and need for orthopedic surgeries (Marcucci et al., 2014). The underlying mechanism(s) of osteonecrosis in GD is not understood. Several mechanisms have been proposed, including disruption of microcirculation by lipid-laden Gaucher macrophages, abnormal red cell morphology leading to ischemia, and osteocyte death (Mikosch and Hughes, 2010). Bone marrow cells in GD exhibit abnormal secretome and osteoblast dysfunction in GD has been linked with accumulating bioactive Gaucher lipid, GlcSph (Mistry et al., 2010; Campeau et al., 2009). There is also evidence of aberrant osteoclast-osteoblast coupling via reduced sphingosine-1-phosphate in GD (Ryu et al., 2006; Ishii et al., 2009). Another emerging player in bone cellular pathology of GD is the damage-associated molecular patterns released by necrotic osteocytes via macrophage-inducible C-type lectin (Mincle), which is known to induce osteoclastogenesis and bone loss (Andreev et al., 2020). In patients with osteonecrosis, Mincle was highly expressed at skeletal sites of osteocyte death and correlated with strong osteoclastic activity (Andreev et al., 2020). GlcCer is a ligand for Mincle, which underscores the complex bone marrow-bone microenvironment in GD and need for optimal therapeutic targeting to prevent disabling AVN.
While AVN occurred frequently in GD in the pre-ERT era (Mistry et al., 2017), introduction of ERT since 1991 has reduced its incidence (Mistry et al., 2009b; Mistry et al., 2009a). However, there are occasional reports of AVN among GD patients receiving ERT (Goker-Alpan, 2011; Potnis et al., 2019; de Fost et al., 2008). Therefore, despite multiplicity of proposed mechanisms underlying AVN in GD, the final pathway likely involves the pathogenic lipids, metabolic inflammation, and lipid-laden Gaucher macrophages. These aberrant pathways are expected to be ameliorated by ERTs and eliglustat SRT but their tissue distribution may have a differential effect (Mistry et al., 2021; Weinreb et al., 2021), for example small molecule SRT vs recombinant MMR-targeted recombinant ERT.
Our study is the first to critically examine outcomes with respect to types (imiglucerase and velaglucerase) and mode of therapy (eliglustat SRT). In experience garnered over 20 years at a single tertiary referral center involving 1382 cumulative years of GD-specific treatments, we found no episode of AVN among eliglustat SRT-treated patients but there were several episodes among patients receiving imiglucerase and velaglucerase ERT. Unexpectedly, we found compared to imiglucerase ERT, patients receiving velaglucerase ERT had 4.7 odds ratio of AVN (95% CI, 1.67–13.07, p=0.003). The basis for this apparent differential effectiveness to prevent AVN is not known. It should be kept in mind that imiglucerase and velaglucerase are not bioidentical. They differ in glycan residues and have minor amino acid changes. Gene expression analysis in mice infused with these enzymes result in different transcriptional profiles (Dasgupta et al., 2013). Moreover, velaglucerase have greater number of mannose residues compared to imiglucerase (Tekoah, 2013). Theoretically, greater clearance by the liver and spleen via mannose receptors in macrophages of these organs could result in less delivery to the bone marrow. Additionally, imiglucerase have been shown to reverse osteoblast defect in cell cultures even though osteoblasts do not exhibit mannose receptors (Panicker et al., 2018). Our findings underscore the need for investigation of this topic in registry setting such as the Gaucher Outcomes Survey (GOS) that monitor long-term outcomes of velaglucerase ERT (ClinicalTrials.gov: NCT03291223). A phase 4 study on bone outcomes was recently completed, and its results will be relevant (ClinicalTrials.gov: NCT02574286) although the primary end-point for the trial appears to be bone density only. During our study, we did not have any episodes of AVN among patients treated with eliglustat SRT. This is in keeping with strikingly low episodes of AVN in extensive clinical trials (Cox et al., 2023). In the ENGAGE placebo-controlled trial, only one episode of AVN occurred in patient on placebo (Mistry et al., 2021; Cox et al., 2023).
Our results advance optimal management of patients with GD based on their biomarker profile. We found that other significant predictors of AVN while receiving treatment included patients with history of AVN prior to initiation of therapy, p.Ser409Asp/other GBA genotype and serum GlcSph level. We did not find any association of splenectomy with occurrence of AVN while on treatment. Some studies have suggested association of AVN with splenectomy (Mistry et al., 2009b) but studies in longitudinally followed patients in UK showed AVN occurrence frequently preceded splenectomy suggesting that both AVN and need for splenectomy in pre-ERT era were indicators of severe disease (Deegan et al., 2011).
In our cohort, GBA genotype had a significant effect on the risk for developing osteonecrosis during treatment. Patients who were heteroallelic for p.Asp409Ser were 10 times more likely than p.Asp409Ser homozygous patients to develop osteonecrosis during treatment. In contrast, p.Asp409Ser/p.Asp409Ser appears to be protective against developing osteonecrosis, underscored by the fact that 51% of our cohort were homozygous for p.Asp409Ser mutation, among whom only one patient developed AVN during treatment. Another significant risk factor for developing AVN on treatment was previous history of AVN prior to treatment initiation.
The biomarkers of GD, chitotriosidase and GlcSph, are reduced by ERT and eliglustat SRT (Murugesan et al., 2016). Of the therapies we examined, we found eliglustat to be most effective in reducing serum GlcSph compared to ERTs (imiglucerase>velaglucerase). We did not find any association of residual chitotriosidase and AVN. This is in keeping with other reports (Khan et al., 2012). In our study we found residual serum GlcSph to be significantly associated with risk of AVN. Residual GlcSph level refers to serum concentration measured in sample taken at close proximity to the onset of AVN (but not levels prior to initiation of treatment). For the first time, our data demonstrate the significance of residual biomarker level which should aid patient stratification for risk of AVN among patients receiving treatment. We used a dual cut-off strategy for serum level of GlcSph to stratify patients for the risk of AVN while receiving treatment in GD patients. There were no episodes of AVN when GlcSph level was less than 21.7 ng/ml with a sensitivity of 100% (95% CI, 79.4–100%) and specificity 24.6%. In contrast, GlcSph level of 77.64 ng/ml has sensitivity of 81.2% (95% CI, 54.4–96%) and specificity of 82.8% (95% CI, 80.7–84.8%) for association with AVN in GD patients receiving treatment. Therefore, our findings permit AVN risk stratification based on GlcSph levels into three groups (Table 4): patients with low risk: GlcSph<21.7 ng/ml, patients with intermediate risk: 21.8 ng/ml<GlcSph<77.64 ng/ml, and patients at high risk: GlcSph>77.64 ng/ml.
Table 4
Serum glucosylsphingosine (GlcSph) levels according to probabilities for avascular osteonecrosis (AVN) occurrence while on treatment with dual cut-offs to stratify patients for AVN risk.
Residual serum GlcSph levels were used to stratify risk of AVN among patients receiving treatment. Our findings permit AVN risk stratification based on GlcSph levels into three groups patients with low risk: GlcSph<21.7 ng/ml, patients with intermediate risk: 21.8ng/ml<GlcSph< 77.64 ng/ml, and patients at high risk: GlcSph>77.64 ng/ml.
| AVN on treatment | GlcSph (ng/ml) | Sensitivity(95% CI) | Specificity(95% CI) | +Likelihood ratio |
|---|---|---|---|---|
| Low risk | <21.7 | 100 (79.4–100) | 24.63 (22.3–27.0) | 1.33 |
| Intermediate risk | 21.8–77.6 | 89 (61.3–98) | 56.9 (54–62.5) | 2.36 |
| High risk | >77.64 | 81.25 (54.4–96) | 82.78 (80.7–84.8) | 4.72 |
These findings suggest that it is prudent to aim to achieve GlcSph levels <21.8 ng/ml as a therapeutic goal, that is, <21.8-fold above normal. In practice, the significance of considering these GlcSph levels is greatly enhanced by considering its context of use regarding other risk factors. For example, as shown in Figure 2B, in patients with at least one of delineated risk factors in our study that is compound heterozygosity for p.Asn409Ser, history of AVN prior to treatment or velaglucerase ERT, sensitivity for GlcSph level at 77.64 ng/ml increases to 87.5% (Figure 2B). In patients who harbor at least two of these risk factors, GlcSph level of 77.14 ng/ml has sensitivity of 92.9% and specificity of 78.8% to rule in the probability of AVN on ERT (Figure 2C). In patients with all three risk factors, GlcSph level of 71.8 ng/ml is 100% sensitive to support the probability of AVN with specificity of 82.4% (Figure 2D).
Our findings are not an indication to change ERTs, as we recognize many patients are benefiting from both imiglucerase and velaglucerase. However, our experience suggests that it is unwise for empirical changes in types of ERTs by third parties (Barranger et al., 2014). Rather, our findings help to elevate optimal management of GD from prevalent practice of monitoring blood counts with or without biomarkers and occasional imaging to a higher level of risk stratification to identify high-risk patients who would benefit from closer monitoring and treatment optimization. Our study is not without limitations. First, it is a single center study, however, the uniform protocol for comprehensive evaluation and long-term follow-up of individual patients are significant strengths. Second, our center is a tertiary referral center, and a referral bias could have enriched patients with AVN, however, this potential bias would apply across our entire patient population. It will be important to examine the GOS which captures data on outcomes of velaglucerase ERT. Hitherto, reports from GOS have iteratively reported only hematological and visceral outcomes, frequently conflating outcomes from multiple ERTs under a generic term ERT (Hughes et al., 2022). It behooves on the investigators to build incremental evidence of efficacy, instead of iterative reports of end-points used in primary trials. It should be noted that in 2014, a study was initiated to assess bone outcomes on velaglucerase ERT (ClinicalTrials.gov: Identifier: NCT02574286), however, there are no reports to date from this study and end-points do not include reduction of AVN incidence.
In conclusion, our study demonstrates residual risk of AVN on GD patients receiving therapy. Independent risk factors for AVN while patients were receiving therapy were pAsp409Ser/other GBA mutation, pre-ERT history of AVN, serum GlcSph level, and velaglucerase ERT. Our results will aid optimal monitoring of GD patients, help enrich clinical trials of rare heterogeneous GD, and stimulate comparative effectiveness analysis in the era of multiple therapies.
Data availability
This observational study is approved by Yale University IRB and each patient provided informed consent. The patients have not provided consent to sharing their data with other investigators. Interested academic, non-commercial researchers can contact the Senior Corresponding author, Dr Pramod Mistry at Pramod.mistry@yale.edu to discuss the request to access original data. They do not need to apply or submit a project proposal. All statistical analyses were performed with SPSS version 28 (SPSS Inc, Chicago, IL, USA). MedCalc version 20.026 was used for ROC curve analysis and graphs were plotted by GraphPad Prism version 9.3.1.We do not have consent to share individual patient data. Even de-identified data risks identification through age and GBA genotype information, thus violating HIPPA patient confidentiality. Upon request to the Senior Corresponding author, the PI, we will share processed version of datasets.
References
-
Osteocyte necrosis triggers Osteoclast-mediated bone loss through macrophage-inducible C-type lectinThe Journal of Clinical Investigation 130:4811–4830.https://doi.org/10.1172/JCI134214
-
Position statement: national Gaucher foundation medical advisory boardAmerican Journal of Hematology 89:457–458.https://doi.org/10.1002/ajh.23687
-
The human Chitotriosidase Gene: nature of inherited enzyme deficiencyThe Journal of Biological Chemistry 273:25680–25685.https://doi.org/10.1074/jbc.273.40.25680
-
Gaucher disease: recommendations on diagnosis, evaluation, and monitoringArchives of Internal Medicine 158:1754–1760.https://doi.org/10.1001/archinte.158.16.1754
-
Competing for the treasure in exceptionsAmerican Journal of Hematology 88:163–165.https://doi.org/10.1002/ajh.23399
-
ConferenceGaucher Disease, a Century of Delineation and ResearchProceedings of the First International Symposium on Gaucher Disease. pp. 22–24.
-
Long-read single molecule real-time (SMRT) sequencing of Gba1 locus in Gaucher disease national cohort from Argentina reveals high frequency of complex allele underlying severe Skeletal phenotypes: collaborative study from the Argentine group for diagnosis and treatment of Gaucher diseaseMolecular Genetics and Metabolism Reports 29:100820.https://doi.org/10.1016/j.ymgmr.2021.100820
-
Therapeutic approaches to bone pathology in Gaucher disease: past, present and futureMolecular Genetics and Metabolism 104:438–447.https://doi.org/10.1016/j.ymgme.2011.08.004
-
BookGaucher diseaseIn: Valle DL, Antonarakis S, Ballabio A, Beaudet AL, Mitchell GA, editors. The Online Metabolic and Molecular Bases of Inherited Disease. McGraw-Hill Education. pp. 1–64.
-
Gaucher disease in bone: from to practice pathophysiologyJournal of Bone and Mineral Research 34:996–1013.https://doi.org/10.1002/jbmr.3734
-
Gaucher disease and bone manifestationsCalcified Tissue International 95:477–494.https://doi.org/10.1007/s00223-014-9923-y
-
An overview on bone manifestations in Gaucher diseaseWiener Medizinische Wochenschrift 160:609–624.https://doi.org/10.1007/s10354-010-0841-y
-
Understanding the natural history of G Aucher diseaseAmerican Journal of Hematology 90 Suppl 1:S6–S11.https://doi.org/10.1002/ajh.24055
-
Clinical outcomes after 4.5 years of Eliglustat therapy for Gaucher disease type 1: phase 3 ENGAGE trial final resultsAmerican Journal of Hematology 96:1156–1165.https://doi.org/10.1002/ajh.26276
-
Glucosylsphingosine is a key biomarker of Gaucher diseaseAmerican Journal of Hematology 91:1082–1089.https://doi.org/10.1002/ajh.24491
-
Clonal immunoglobulin against Lysolipids in the origin of myelomaNew England Journal of Medicine 374:555–561.https://doi.org/10.1056/NEJMoa1508808
-
Glucosylsphingosine accumulation in tissues from patients with Gaucher disease: correlation with phenotype and genotypeMolecular Genetics and Metabolism 76:262–270.https://doi.org/10.1016/s1096-7192(02)00117-8
-
Bone manifestations in Neuronopathic Gaucher disease while receiving high-dose enzyme replacement therapyMolecular Genetics and Metabolism 126:157–161.https://doi.org/10.1016/j.ymgme.2018.11.004
-
Overview of immune abnormalities in lysosomal storage disordersImmunology Letters 188:79–85.https://doi.org/10.1016/j.imlet.2017.07.004
-
Expanding the clinical utility of Glucosylsphingosine for Gaucher diseaseJournal of Inherited Metabolic Disease 43:558–563.https://doi.org/10.1002/jimd.12192
-
Monitoring of Gaucher patients with a novel Chitotriosidase assayClinica Chimica Acta 381:136–139.https://doi.org/10.1016/j.cca.2007.02.042
-
ConferenceAvascular necrosis in untreated patients with type 1 Gaucher diseaseMolecular Genetics and Metabolism.
-
Safety and efficacy of Velaglucerase ALFA in Gaucher disease type 1 patients previously treated with ImigluceraseAmerican Journal of Hematology 88:172–178.https://doi.org/10.1002/ajh.23383
Article and author information
Author details
Funding
Sanofi Genzyme (LSD Training Fellowship from Sanofi to MB)
- Mohsen Basiri
The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
Acknowledgements
We thank our patients for the opportunity to provide their Gaucher-related care and for their participation in our studies. MB is supported by Lysosomal Disease Fellowship from Sanofi.
Ethics
Human subjects: All participants were enrolled in our observational studies approved by Yale's IRB. Patients also were provided with verbal explanations and their data were collected after signing consent forms. HIC#0209021074HIC#1005006783.
Copyright
© 2023, Basiri et al.
This article is distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use and redistribution provided that the original author and source are credited.
Metrics
-
- 1,862
- views
-
- 394
- downloads
-
- 12
- citations
Views, downloads and citations are aggregated across all versions of this paper published by eLife.
Citations by DOI
-
- 12
- citations for umbrella DOI https://doi.org/10.7554/eLife.87537
Download links
A two-part list of links to download the article, or parts of the article, in various formats.
Downloads (link to download the article as PDF)
Open citations (links to open the citations from this article in various online reference manager services)
Cite this article (links to download the citations from this article in formats compatible with various reference manager tools)
Osteonecrosis in Gaucher disease in the era of multiple therapies: Biomarker set for risk stratification from a tertiary referral center
eLife 12:e87537.
https://doi.org/10.7554/eLife.87537




{kind=link}
{kind=link}
{kind=link}